IPLab:Lab 7:Osteosarcoma
Contents
Clinical Summary[edit]
This 14-year-old male first experienced mild pain in the left knee after playing baseball, approximately two months ago. The pain persisted in an intermittent fashion until approximately two weeks prior to admission, when the pain increased significantly and was accompanied by marked swelling and loss of motion. He also had decreased appetite, lethargy, and a 10-pound weight loss. On physical examination, the left knee was enlarged diffusely, firm, and non-tender. Radiographic and biopsy results confirmed a diagnosis of osteosarcoma. The patient underwent surgical removal of the distal femur and knee with placement of a prosthetic knee joint and bone grafts.
The distal diaphysis of the femur and adjacent soft tissues were involved in a 15 x 10 x 10-cm mass. The cut surface of the mass was fleshy white, with focal areas of hemorrhage.
Images[edit]

This is a photograph of the patient prior to surgery. Note the marked swelling of the knee.

This is a radiograph showing the tumor in the distal femur.
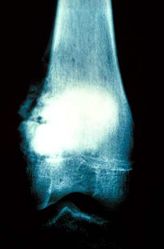
This is another view of the tumor in the distal femur.
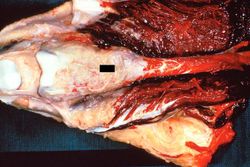
This is a gross photograph of the surgical specimen with tissue dissected away to demonstrate the tumor mass.

These are cut sections of the distal femur containing the tumor. The periosteal involvement is evident from this picture (arrows).

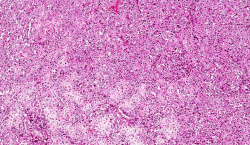
This is a low-power photomicrograph of decalcified histologic section from this tumor. Note the blue color (cell nuclei stain blue) of much of this section indicating the increased cellularity of the tumor.
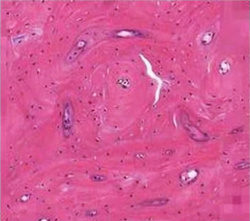
This is a photomicrograph of a decalcified histologic section from normal bone. Compare this normal morphology to the subsequent images of bone in this case of osteosarcoma.
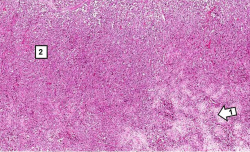
This is a higher-power photomicrograph of decalcified histologic section from this tumor. There are areas of osteoid (1) and cellular areas (2).
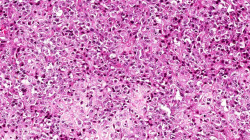
This is a higher-power photomicrograph of decalcified histologic section showing the cellularity of the tumor.
This higher-power photomicrograph demonstrates the cellular growth pattern. Note that the cells are pleomorphic and anaplastic.
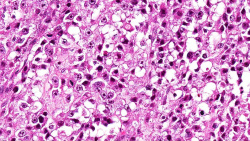
This high-power photomicrograph demonstrates the anaplastic cell morphology.
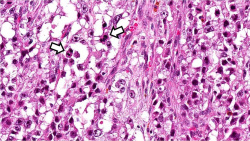
This is a high-power photomicrograph of the tumor demonstrating the anaplastic cell morphology and mitotic figures (arrows).












Virtual Microscopy[edit]
Study Question[edit]
Additional Resources[edit]
Reference[edit]
Journal Articles[edit]
- Wittig JC, Bickels J, Priebat D, Jelinek J, Kellar-Graney K, Shmookler B, Malawer MM. Osteosarcoma: a multidisciplinary approach to diagnosis and treatment. Am Fam Physician 2002 Mar 15;65(6):1123-32.
- Miller SL, Hoffer FA. Malignant and benign bone tumors. Radiol Clin North Am 2001 Jul;39(4):673-99.
Images[edit]
The normal fibrinogen level is 184 to 412 mg/dL.