IPLab:Lab 7:Lip SCC
Contents
Clinical Summary[edit]
This 63-year-old white male had recurrent thickening and scaling of the lower lip for two years. In recent months, it had undergone ulceration and progressive enlargement. The lesion was excised by a wedge resection.
The biopsy specimen was triangular in shape; the upper part was covered by mucosa and the lower part by skin. At the junction of the mucosa and skin there was a 2 x 1.4 cm oval shaped superficial lesion which was flat, firm, and had raised borders. The base was orange.
Images[edit]

This is a pre-op photograph of this patient with an ulcerated lesion on his lip (arrow). Also note that the lip is somewhat thickened. The area for surgical excision is delineated by black marker.
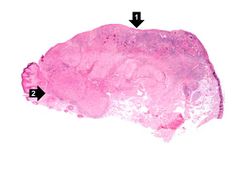
This is a low-power photomicrograph of squamous cell carcinoma of the lip. Note focal ulceration (1) and tumor infiltration at the vermilion border (2).
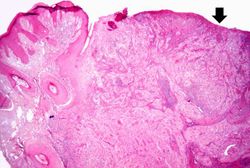
This photomicrograph shows a large area of ulceration (arrow) with underlying congestion and hemorrhage. The area of ulceration is adjacent to an area of tumor infiltration.
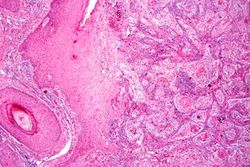
This is a higher-power photomicrograph of the well-differentiated squamous cell carcinoma and the inflammatory cell infiltration.
This is a higher-power photomicrograph of infiltrating squamous cell carcinoma and inflammatory cells.
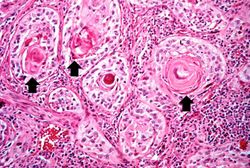
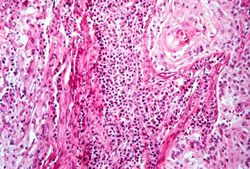
This is a high power photomicrograph of the well-differentiated squamous cell carcinoma. Note the intracytoplasmic keratinization which gives the cells a glassy appearance. The focal accumulations of keratinized cells are called keratin pearls (arrows).
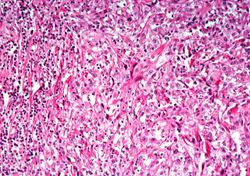
This is a high power photomicrograph of a poorly-differentiated area of tumor. Note the spindle-shaped cells and the irregular pattern of growth.
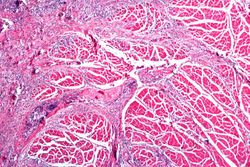
This is a section of muscle tissue from this biopsy of the lip. Note that the squamous cell carcinoma has infiltrated into the muscle tissue. There are also inflammatory cells within this area of tumor infiltration.








Virtual Microscopy[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Head and Neck Cutaneous Squamous Cell Carcinoma
- Merck Manual: Overview of Skin Cancer
- Merck Manual: Squamous Cell Carcinoma
Journal Articles[edit]
- Guenthner ST, Hurwitz RM, Buckel LJ, Gray HR. Cutaneous squamous cell carcinomas consistently show histologic evidence of in situ changes: a clinicopathologic correlation. J Am Acad Dermatol 1999 Sep;41(3 Pt 1):443-8.
- Ling S, Hu Z, Yang Z, Yang F, Li Y, Lin P, Chen K, Dong L, Cao L, Tao Y, Hao L, Chen Q, Gong Q, Wu D, Li W, Zhao W, Tian X, Hao C,Hungate EA, Catenacci DV, Hudson RR, Li WH, Lu X, Wu CI. Extremely high genetic diversity in a single tumor points to prevalence of non-Darwinian cell evolution.. Proc Natl Acad Sci U S A 2015 Nov 24;112(47):E6496-505.
Images[edit]
Related IPLab Cases[edit]
- Lab 7: Esophagus: Squamous Cell Carcinoma
- Lab 7: Breast: Infiltrating Ductal Carcinoma
- Lab 7: Lung: Bronchogenic Carcinoma
- Lab 7: Colon: Adenocarcinoma
- Lab 7: Lung & Liver: Metastatic Adenocarcinoma
The normal fibrinogen level is 184 to 412 mg/dL.