IPLab:Lab 7:Adenocarcinoma
Contents
Clinical Summary[edit]
Approximately four months prior to admission, this 68-year-old male began having "sharp, shooting pains" in the lower abdomen. On admission a CT scan showed a mass in the transverse colon. The patient refused to undergo a laparotomy and declined further treatment. Six months later he returned with severe abdominal pain and a colectomy was performed.
The segment of colon contained numerous polyps and an annular tumor which was 6.7 cm in diameter. Endoscopic examination of the ascending colon revealed two more polyps which were removed.
Images[edit]
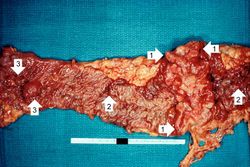
This is a gross photograph of the adenoma from the surgical specimen in this case. Note the large, ulcerated, fungating annular (encircling) carcinoma (1) with areas of hemorrhage (2). Also note the adenomatous polyps (3).

This is a closer view of the previous image demonstrating the raised, annular carcinoma (arrows).
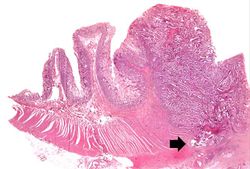
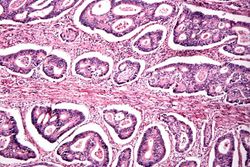
This photomicrograph of the surgical specimen shows the transition between normal mucosa on the left and carcinoma which is invading the wall of the bowel (arrow).
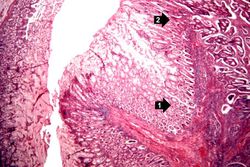
This is a higher-power photomicrograph of the area of transition between the normal (1) and the neoplastic (2) epithelium.
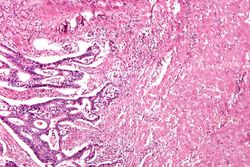
This is a high-power photomicrograph of tumor cells invading the underlying muscularis.
This is a high-power photomicrograph of tumor cells forming glands.
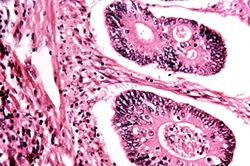
This is a high-power photomicrograph of tumor cells forming glands.

This gross photograph from another case demonstrates an ulcerated adenocarcinoma (arrows) at the rectosigmoid junction.

This is a segment of distal colon from another case. Note the annular tumor that severely compromises the lumen of the colon. There is dilation of the colon proximal to the tumor.









Virtual Microscopy[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Imaging in Adenocarcinoma of the Colon
- eMedicine Medical Library: Colon Adenocarcinoma
- Merck Manual: Colorectal Cancer
Journal Articles[edit]
- Yuen ST, Wong MP, Chung LP, Chan SY, Cheung N, Ho J, Leung SY. Up-regulation of lysozyme production in colonic adenomas and adenocarcinomas. Histopathology 1998 Feb;32(2):126-32.
- Strum WB. Colorectal Adenomas. NEJM 2016 March 17 374:1065-1075.
Images[edit]
Related IPLab Cases[edit]
- Lab 7: Lung & Liver: Metastatic Adenocarcinoma
- Lab 7: Lip: Squamous Cell Carcinoma
- Lab 7: Esophagus: Squamous Cell Carcinoma
- Lab 7: Breast: Infiltrating Ductal Carcinoma
- Lab 7: Lung: Bronchogenic Carcinoma
Melena is the passage of digested blood in the feces.