Difference between revisions of "IPLab:Lab 6:Scleroderma"
(Created page with "== Images == <gallery heights="250px" widths="250px"> File:IPLab6Scleroderma1.jpg|This is a gross photograph of cut section of the lungs from this patient. Note the extensive ...") |
(→Autopsy Findings) |
||
| (14 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
| + | == Clinical Summary == | ||
| + | This 29-year-old black female had a history of scleroderma involving the lung, kidney, heart, and skin. Her main clinical problems centered on her restrictive lung disease. She was able to live at home with supplemental oxygen but recently she had developed edema, chest pain, weakness, light-headedness, and a loss of appetite. The patient was admitted to the hospital with a working diagnosis of congestive heart failure brought on by her lung disease. Echocardiographic evaluation revealed a pericardial effusion that was tapped. Soon after this procedure her respiratory status degenerated and she required intubation. Despite aggressive supportive treatment for her cardiac and pulmonary problems, she could not be weaned from the ventilator. Two weeks after admission she became febrile and Gram positive cocci were isolated from sputum culture. She was placed on antibiotics but her condition deteriorated and she developed bradycardia followed by electromechanical dissociation (EMD). | ||
| + | |||
| + | Upon opening the thorax at autopsy there was 600 cc of cloudy serous fluid in each hemithorax and 100 cc of similar fluid in the pericardial sac. The heart weighed 530 grams and there was thickening of both the left and right ventricular walls. The liver weighed 1880 grams and was congested. The spleen weighed 200 grams and was also congested. The combined lung weight was 1875 grams; the lungs were markedly fibrotic with severe emphysema. In addition, dermal thickening was evident throughout the body and the wall of the esophagus was thickened and firm. | ||
| + | |||
== Images == | == Images == | ||
<gallery heights="250px" widths="250px"> | <gallery heights="250px" widths="250px"> | ||
| Line 7: | Line 12: | ||
File:IPLab6Scleroderma5.jpg|This is a gross photograph of the heart from this case. There is thickening of the left ventricular wall and some thickening of the right ventricle as well. | File:IPLab6Scleroderma5.jpg|This is a gross photograph of the heart from this case. There is thickening of the left ventricular wall and some thickening of the right ventricle as well. | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Virtual Microscopy == | ||
| + | === Lung: Scleroderma === | ||
| + | <peir-vm>IPLab6Scleroderma</peir-vm> | ||
| + | |||
| + | === Normal Lung === | ||
| + | <peir-vm>UAB-Histology-00107</peir-vm> | ||
| + | |||
| + | === Skin: Scleroderma === | ||
| + | <peir-vm>IPLab6Scleroderma_Skin</peir-vm> | ||
| + | |||
| + | === Normal Skin === | ||
| + | <peir-vm>UAB-Histology-00004</peir-vm> | ||
| + | |||
| + | == Study Questions == | ||
| + | * <spoiler text="What organs are usually affected in patients with scleroderma (progressive systemic sclerosis, PSS)?">Skin, gastrointestinal tract, kidneys, heart, muscles, and lungs.</spoiler> | ||
| + | * <spoiler text="What are the common clinical ramifications of PSS?">The striking cutaneous involvement is the primary clinical problem in many early cases. Raynaud's phenomenon, dysphagia due to esophageal fibrosis and hypomotility, abdominal pain, and intestinal obstruction are caused by fibrosis and scaring of these tissues. The respiratory problems are caused by pulmonary fibrosis. Chronic pulmonary fibrosis may lead to right-sided heart failure.</spoiler> | ||
| + | * <spoiler text="What is the etiology of PSS?">The exact etiology of PSS is not known. PSS is associated with excessive fibrosis, changes in the microvasculature, and a variety of immunologic abnormalities including T cell and humoral abnormalities that either cause or are caused by cytokines. The antigens that trigger the immune response have not been identified.</spoiler> | ||
| + | * <spoiler text="What is the CREST syndrome?">Some patients with a milder form of PSS may demonstrate the CREST syndrome. CREST stands for calcinosis, Raynaud’s phenomenon, esophageal dysfunction, sclerodactyly, telangiectasia, and the presence of anticentromere antibodies. These patients usually have less skin involvement of skin, and the more serious visceral problems do not develop until later in the course of the disease. | ||
| + | </spoiler> | ||
| + | |||
| + | == Additional Resources == | ||
| + | === Reference === | ||
| + | * [http://emedicine.medscape.com/article/331864-overview eMedicine Medical Library: Scleroderma] | ||
| + | * [http://emedicine.medscape.com/article/1064663-overview eMedicine Medical Library: CREST Syndrome] | ||
| + | * [http://www.merckmanuals.com/professional/musculoskeletal_and_connective_tissue_disorders/autoimmune_rheumatic_disorders/systemic_sclerosis.html Merck Manual: Systemic Sclerosis] | ||
| + | |||
| + | === Images === | ||
| + | * [{{SERVER}}/library/index.php?/tags/2144-scleroderma PEIR Digital Library: Scleroderma Images] | ||
| + | |||
| + | == Related IPLab Cases == | ||
| + | * [[IPLab:Lab 2:Hypertrophy|Lab 2: Heart: Myocardial Hypertrophy]] | ||
| + | * [[IPLab:Lab 5:α1 Antitrypsin Deficiency|Lab 5: Lung: α1-Antitrypsin Deficiency]] | ||
{{IPLab 6}} | {{IPLab 6}} | ||
[[Category: IPLab:Lab 6]] | [[Category: IPLab:Lab 6]] | ||
Latest revision as of 23:38, 8 July 2020
Contents
Clinical Summary[edit]
This 29-year-old black female had a history of scleroderma involving the lung, kidney, heart, and skin. Her main clinical problems centered on her restrictive lung disease. She was able to live at home with supplemental oxygen but recently she had developed edema, chest pain, weakness, light-headedness, and a loss of appetite. The patient was admitted to the hospital with a working diagnosis of congestive heart failure brought on by her lung disease. Echocardiographic evaluation revealed a pericardial effusion that was tapped. Soon after this procedure her respiratory status degenerated and she required intubation. Despite aggressive supportive treatment for her cardiac and pulmonary problems, she could not be weaned from the ventilator. Two weeks after admission she became febrile and Gram positive cocci were isolated from sputum culture. She was placed on antibiotics but her condition deteriorated and she developed bradycardia followed by electromechanical dissociation (EMD).
Upon opening the thorax at autopsy there was 600 cc of cloudy serous fluid in each hemithorax and 100 cc of similar fluid in the pericardial sac. The heart weighed 530 grams and there was thickening of both the left and right ventricular walls. The liver weighed 1880 grams and was congested. The spleen weighed 200 grams and was also congested. The combined lung weight was 1875 grams; the lungs were markedly fibrotic with severe emphysema. In addition, dermal thickening was evident throughout the body and the wall of the esophagus was thickened and firm.
Images[edit]

This is a gross photograph of cut section of the lungs from this patient. Note the extensive fibrosis of the lung parenchyma.
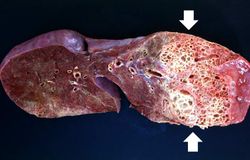
This is a gross photograph of a cut section of one lung from this patient. Note the extensive fibrosis lower lobe (arrows).
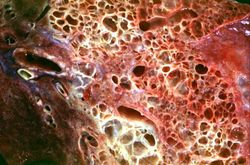
This is a closer view of the cut section of lung from this patient. Note the extensive fibrosis and the severe emphysematous changes.
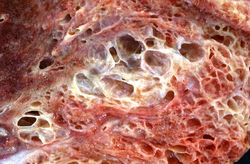
This is a closer view of the cut section of lung from this patient showing the extensive fibrosis and the severe emphysematous change.
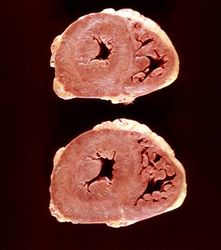
This is a gross photograph of the heart from this case. There is thickening of the left ventricular wall and some thickening of the right ventricle as well.





Virtual Microscopy[edit]
Lung: Scleroderma[edit]
Normal Lung[edit]
Skin: Scleroderma[edit]
Normal Skin[edit]
Study Questions[edit]
- What organs are usually affected in patients with scleroderma (progressive systemic sclerosis, PSS)?
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Scleroderma
- eMedicine Medical Library: CREST Syndrome
- Merck Manual: Systemic Sclerosis
Images[edit]
Related IPLab Cases[edit]
A pericardial effusion is a collection of fluid within the pericardial space.
Bradycardia is defined as a heart rate below 60 beats per minute. A normal heart rate for a neonate is 100 to 160 beats per minute.
EMD is a condition in which the heart's electrical rhythm continues despite the mechanical failure of the myocardium.
A normal heart weighs 300 grams (range: 270 to 360 grams).
A normal liver weighs 1650 grams (range: 1500 to 1800 grams).
The normal spleen weighs 155 grams.
A normal pair of lungs weighs 825 grams (range: 685 to 1050 grams).
Pulmonary emphysema is a condition in which the air spaces distal to the terminal bronchioles are permanently increased in size due to either destruction of the wall or alveolar dilatation.