Difference between revisions of "IPLab:Lab 6:Hashimoto's Thyroiditis"
Seung Park (talk | contribs) |
|||
| Line 17: | Line 17: | ||
File:IPLab6Hashimoto9.jpg|This high-power photomicrograph shows more clearly the lymphocytes and plasma cells surrounding the thyroid gland epithelium. Large, eosinophilic, degenerating thyroid gland cells (Hurthle cells) can be seen in this section (arrows). | File:IPLab6Hashimoto9.jpg|This high-power photomicrograph shows more clearly the lymphocytes and plasma cells surrounding the thyroid gland epithelium. Large, eosinophilic, degenerating thyroid gland cells (Hurthle cells) can be seen in this section (arrows). | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Study Questions == | ||
| + | * <spoiler text="What signs and symptoms in this patient suggest a diagnosis of hypothyroidism and what are some of the other signs and symptoms seen with hypothyroidism?">Fatigue, lethargy, slowed speech, cold intolerance, dry skin, course hair, puffy face, myxedema, slowed reflexes, and diffuse goiter.</spoiler> | ||
| + | * <spoiler text="What is the pathogenesis of Hashimoto’s thyroiditis and how does this disease differ from Grave’s disease or nutritional goiter?">Hashimoto's thyroiditis is characterized by Iymphocytic infiltration of the thyroid gland and production of antibodies that recognize thyroid-specific antigens. It is currently thought that the disease is caused by abnormal suppressor T-lymphocyte function which results in a localized cell-mediated immune response directed toward the thyroid parenchymal cells. The pathogenesis is not completely understood. In contrast Graves' disease is caused by production of antibodies that mimic the action of thyroid-stimulating hormone. Nutritional goiter is caused by iodine deficiency.</spoiler> | ||
| + | * <spoiler text="What are some of the pathologic changes seen in Hashimoto's thyroiditis?">The gland is usually diffusely enlarged, firm, and slightly lobular. The capsule is intact, and the cut surface is light tan and has a slight lobular pattern. Microscopically there is massive infiltration of the thyroid gland by lymphocytes and plasma cells. Germinal centers can often be seen in the gland. Thyroid follicles are usually absent and the few remaining follicles are devoid of colloid.</spoiler> | ||
{{IPLab 6}} | {{IPLab 6}} | ||
[[Category: IPLab:Lab 6]] | [[Category: IPLab:Lab 6]] | ||
Revision as of 15:24, 21 August 2013
Clinical Summary[edit]
This was a 49-year-old woman who complained during her yearly physical examination of tiredness and difficulty concentrating. She attributed these symptoms to stress at work. She had gained weight over the last year and despite warm weather, she felt chilled without a sweater. Family history was significant for hypothyroidism in her mother and older sister. On physical examination she had a pulse of 58 bpm and a blood pressure of 138/88 mm Hg. Examination of her neck disclosed a small thyroid gland with a palpable pyramidal lobe and a firm, bosselated texture. Serum taken at this time demonstrated a total T4 of 7.0 mcg/dL and a TSH of 22.0 mcIU/ml. In addition, antithyroglobulin antibodies were positive at 1:640 and antimicrosomal antibodies were positive at 1:5120. These results supported the clinical impression of hypothyroidism; also, the texture of her thyroid gland and a positive family history suggested an autoimmune etiological factor. She was referred to an endocrinologist for further evaluation; however, before beginning treatment she died suddenly from a ruptured berry aneurysm of the middle cerebral artery.
Autopsy Findings[edit]
At autopsy, significant subarachnoid hemorrhage from the ruptured berry aneurysm was documented. In addition, the thyroid gland was mildly enlarged and firm. On cut section the tissue was slightly pale.
Images[edit]

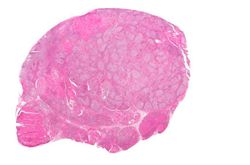
This is a gross photograph of thyroid gland taken at autopsy. The gland is only slightly enlarged and has a firm texture.
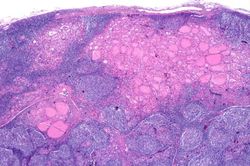
This is a low-power photomicrograph of thyroid from this case. Note that the tissue is more cellular than one would expect and there does not appear to be normal colloid-filled blue spaces in this gland.
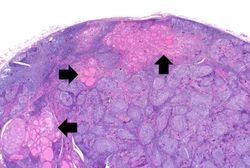
This is a higher-power photomicrograph of thyroid from this case. Note the large number of blue-staining inflammatory cells in this tissue. These cells appear to be forming germinal centers. Some residual thyroid gland tissue can be seen in this section (arrows).
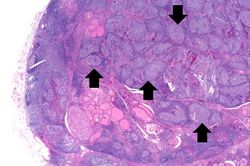
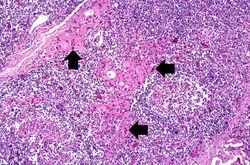
This is another view of thyroid gland filled with inflammatory cells forming germinal centers (arrows).
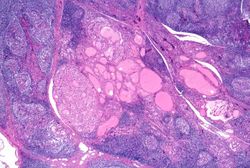
This is a higher-power photomicrograph of thyroid from this case showing the inflammatory cells and the residual thyroid tissue.
This is another higher-power photomicrograph of thyroid from this case showing the inflammatory cells and the residual thyroid tissue.
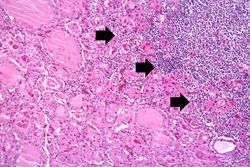
This is a high-power photomicrograph showing the inflammatory cells infiltrating into the residual thyroid tissue (arrows).
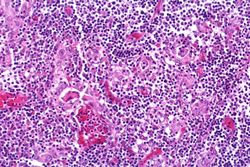
This is a high-power photomicrograph showing the lymphocytes and plasma cells surrounding the thyroid gland epithelium.
This high-power photomicrograph shows more clearly the lymphocytes and plasma cells surrounding the thyroid gland epithelium. Large, eosinophilic, degenerating thyroid gland cells (Hurthle cells) can be seen in this section (arrows).
Study Questions[edit]
A normal pulse rate is 60 to 100 bpm.
A normal blood pressure reading would be 120/80 mm Hg.
Bosselated means covered with rounded protuberances.
A normal T4 level is 4 to 11 mcg/dL.
A normal TSH level is 0.32 to 5.00 mcIU/dL.
Antithyroglobulin antibodies are autoimmune antibodies directed against thyroglobulin. Over half of all patients with Hashimotos thyroiditis have positive titers, although they are also found in other types of thyroiditis.
Antimicrosomal antibodies are autoimmune antibodies directed at the thyroid gland. They are seen in almost all patients with Hashimotos thyroiditis.
Autoimmune disorders involve an immune response directed at the host's own cells.
A berry aneurysm is a small saccular arterial aneurysm usually found at a vessel junction in the circle of Willis. These aneurysms frequently rupture, causing a subarachnoid hemorrhage.