Difference between revisions of "IPLab:Lab 6:Glomerulonephritis"
Seung Park (talk | contribs) |
|||
| Line 18: | Line 18: | ||
File:IPLab6GN10.jpg|For comparison this is an immunofluorescent photomicrograph of a glomerulus from a patient with Goodpasture's syndrome. The linear (arrows) immunofluorescence is characteristic of Goodpasture's syndrome. | File:IPLab6GN10.jpg|For comparison this is an immunofluorescent photomicrograph of a glomerulus from a patient with Goodpasture's syndrome. The linear (arrows) immunofluorescence is characteristic of Goodpasture's syndrome. | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Study Questions == | ||
| + | * <spoiler text="What is the usual clinical course of poststreptococcal glomerulonephritis?">One to two weeks after infection (usually sore throat or skin infection) by certain types of group A beta-hemolytic streptococci, patients develop malaise, fever, nausea, oliguria, and hematuria. Most patients recover with conservative treatment aimed at maintaining sodium and water balance. The renal injury usually resolves with no loss of function.</spoiler> | ||
| + | * <spoiler text="What is the pathogenetic mechanism of poststreptococcal glomerulonephritis?">Patients have elevated antibody titers to streptococcal antigens, decreased complement levels, and accumulations of immune complexes and complement in the glomeruli suggesting immune complex mediated glomerular injury. Some streptococcal antigens (endostreptosin and several cationic antigens) have been demonstrated on the glomerular basement membrane. Thus, it is not known for sure if the glomerular damage is caused by circulating antigen antibody complexes, antibodies attacking streptococcal antigens that are attached to the basement membrane, or a combination of both processes. In any event, antibodies bind to antigens, activate complement, and cause damage to the glomeruli. | ||
| + | </spoiler> | ||
{{IPLab 6}} | {{IPLab 6}} | ||
[[Category: IPLab:Lab 6]] | [[Category: IPLab:Lab 6]] | ||
Revision as of 15:36, 21 August 2013
Clinical Summary[edit]
This 17-year-old white male had end-stage renal disease requiring hemodialysis for 10 years. For the previous four years he had hypertension which slowly increased to about 180/120 mm Hg. Laboratory findings included a greatly elevated BUN and creatinine. He was admitted for bilateral nephrectomy and discharged in satisfactory condition on the 10th postoperative day. He was to be contacted in the future for transplantation.
Autopsy Findings[edit]
The left (97 grams) and right (88 grams) kidneys were of similar appearance. Cortices were pale, diffusely granular with a few 1-2 mm cysts. On being sectioned, the cortex of each kidney was thin (4-5 mm) and pale. Renal medullae were pale yellow-tan in color and there was abundant peripelvic fat. The ureters, pelvis, calyces and hilar vessels showed no abnormalities.
Images[edit]
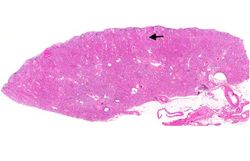
This is a low-power photomicrograph of a saggital section of end stage chronic glomerulonephritis (GN). Note the marked thinning of the cortex (arrow).
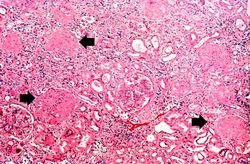
This is a higher-power photomicrograph of hyalinized glomeruli (arrows) and glomeruli with thick basement membranes.
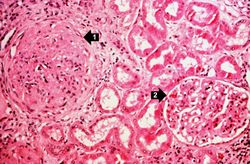
This is a higher-power photomicrograph of hyalinized glomeruli (1) and glomeruli with thickened basement membranes (2).
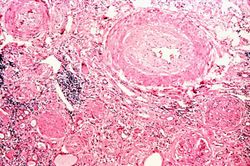
This is a photomicrograph of interstitial and vascular lesions in end stage renal disease.
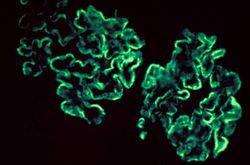
This is an immunofluorescent photomicrograph of granular membranous immunofluorescence (immune complex disease). The antibody used for these studies was specific for IgG.
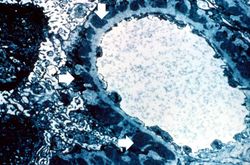
This is an electron micrograph of subepithelial granular electron dense deposits (arrows) which correspond to the granular immunofluorescence seen in the previous image.
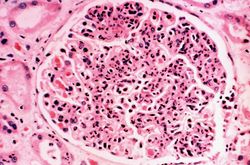
This is a photomicrograph of a glomerulus from another case with acute poststreptococcal glomerulonephritis. In this case the immune complex glomerular disease is ongoing with necrosis and accumulation of neutrophils in the glomerulus.
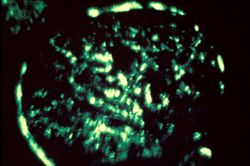
This immunofluorescent photomicrograph of a glomerulus from a case of acute poststreptococcal glomerulonephritis shows a granular immunofluorescence pattern consistent with immune complex disease. The primary antibody used for this staining was specific for IgG; however antibodies for complement would show a similar pattern.
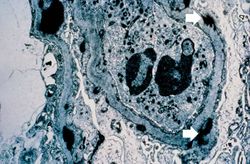
This electron micrograph demonstrates scattered subepithelial dense deposits (arrows) and a polymorphonuclear leukocyte in the lumen.
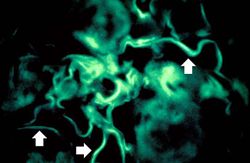
For comparison this is an immunofluorescent photomicrograph of a glomerulus from a patient with Goodpasture's syndrome. The linear (arrows) immunofluorescence is characteristic of Goodpasture's syndrome.










Study Questions[edit]
A normal alkaline phosphatase is 39 to 117 U/L.
These tests are measures of kidney function. High levels mean low function.
A normal kidney weighs 157 grams (range: 115 to 220 grams).
A normal kidney weighs 157 grams (range: 115 to 220 grams).
Oliguria is the occurrence of decreased urine output.
Hematuria is the presence of blood in the urine.