Difference between revisions of "IPLab:Lab 6:Chronic Rejection"
Seung Park (talk | contribs) |
|||
| Line 25: | Line 25: | ||
* <spoiler text="Why does this case of chronic transplant rejection have cellular infiltrate and even some neutrophils (indicating acute inflammation)?">There is often ongoing rejection even in cases of long term transplant. This case and the images from the case of chronic rejection that was removed during an attack of acute rejection demonstrate the continuing ongoing nature of the rejection process.</spoiler> | * <spoiler text="Why does this case of chronic transplant rejection have cellular infiltrate and even some neutrophils (indicating acute inflammation)?">There is often ongoing rejection even in cases of long term transplant. This case and the images from the case of chronic rejection that was removed during an attack of acute rejection demonstrate the continuing ongoing nature of the rejection process.</spoiler> | ||
* <spoiler text="What role do humoral antibodies play in chronic transplant rejection?">There is some controversy over this point. Some people think that since antibodies can be demonstrated in the vascular lesions (the intimal proliferation), these must be antibody-mediated. This is not necessarily true but the classic dogma is that chronic vascular rejection is both antibody-mediated and cell-mediated.</spoiler> | * <spoiler text="What role do humoral antibodies play in chronic transplant rejection?">There is some controversy over this point. Some people think that since antibodies can be demonstrated in the vascular lesions (the intimal proliferation), these must be antibody-mediated. This is not necessarily true but the classic dogma is that chronic vascular rejection is both antibody-mediated and cell-mediated.</spoiler> | ||
| + | |||
| + | == Additional Resources == | ||
| + | === Reference === | ||
| + | * [http://emedicine.medscape.com/article/429314-overview eMedicine Medical Library: Assessment and Management of the Renal Transplant Patient] | ||
| + | * [http://emedicine.medscape.com/article/430128-overview eMedicine Medical Library: Renal Transplantation] | ||
| + | * [http://emedicine.medscape.com/article/241640-overview eMedicine Medical Library: Malignant Hypertension] | ||
| + | * [www.merckmanuals.com/professional/cardiovascular_disorders/hypertension/hypertensive_emergencies.html Merck Manual: Hypertensive Emergencies] | ||
| + | * [http://www.merckmanuals.com/professional/genitourinary_disorders/renal_failure/chronic_kidney_disease.html Merck Manual: Chronic Kidney Disease] | ||
| + | * [http://www.merckmanuals.com/professional/genitourinary_disorders/renal_replacement_therapy/hemodialysis.html Merck Manual: Hemodialysis] | ||
| + | * [http://www.merckmanuals.com/professional/immunology_allergic_disorders/transplantation/kidney_transplantation.html Merck Manual: Kidney Transplantation] | ||
| + | |||
| + | === Journal Articles === | ||
| + | * Matas AJ. [http://www.ncbi.nlm.nih.gov/pubmed/11272615 Impact of acute rejection on development of chronic rejection in pediatric renal transplant recipients]. ''Pediatr Transplant'' 2000 May;4(2):92-9. | ||
| + | |||
| + | === Images === | ||
| + | * [http://peir.path.uab.edu/library/index.php?/tags/2146-rejection PEIR Digital Library: Rejection Images] | ||
| + | * [http://library.med.utah.edu/WebPath/IMMHTML/IMMIDX.html#4 WebPath: Transplant Rejection] | ||
{{IPLab 6}} | {{IPLab 6}} | ||
[[Category: IPLab:Lab 6]] | [[Category: IPLab:Lab 6]] | ||
Revision as of 03:59, 23 August 2013
Contents
Clinical Summary[edit]
This 39-year-old male had malignant hypertension with malignant nephrosclerosis, progressing to chronic renal failure. He underwent a bilateral nephrectomy for control of his hypertension and received a cadaveric renal transplant. He did well, although he developed diabetes mellitus and had persistent, but less severe controllable hypertension. Two years following transplantation he was admitted to the hospital for control of his hypertension and evaluation of his chronic rejection. Initial blood pressure while in the hospital was in the range of 160/110 to 160/100 mm Hg. He was placed on a more intensive hypertension regimen, and he gradually became normotensive. He received one hemodialysis treatment prior to discharge. At the time of discharge, his blood pressure was 100 to 110 over 60 to 70 and he was doing well on dialysis. His BUN was 113 mg/dL and creatinine 5.2 mg/dL, and he had a hematocrit (PCV) of 27%. The patient was again admitted one month later for evaluation of azotemia and for control of his hypertension. It was felt that his chronic rejection was end-stage and that he would have to be dialyzed periodically. He was put on a renal failure diet, and over the period of his hospitalization, his BUN and creatinine finally stabilized at high levels. He tolerated dialysis well, and a transplant nephrectomy was done at 2 1/2 years post transplant. At the time of discharge, the patient's BUN was 78 mg/dL, creatinine 3.6 mg/dL, WBC 5000 cells/cmm, and the PCV was 26%.
Autopsy Findings[edit]
The kidney weighed 215 grams and was covered by a thick capsule, which was partially adherent to the cortex, but could be stripped from the kidney with slight difficulty. The calyces and pelvis of the kidney appeared normal. The vessels were not prominent. The renal arteries and vein appeared normal.
Images[edit]
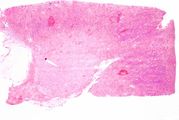
This is a low-power photomicrograph of the kidney from this case of chronic transplant rejection. Note the focal areas of hemorrhage and inflammatory cell infiltrate in this section.
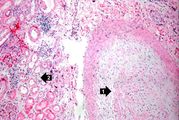
This is a higher-power photomicrograph of kidney containing a section of blood vessel that demonstrates a marked neointimal proliferative response (1). In this case the lumen of the artery is obliterated. Also note the cellular infiltrate in the interstitium of the kidney (2) and the paucity of tubules.
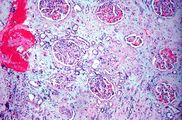
This is a photomicrograph of kidney with a focal area of hemorrhage around a small blood vessel (left) and congestion of the glomeruli. Note that there is a marked loss of renal tubules throughout this section with replacement by fibrous connective tissue. Also note the cellularity of the glomeruli.
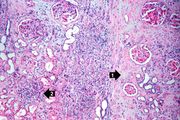
This is another area of renal cortex similar to the previous image. Note the fibrosis (1) and loss of renal tubules throughout this section. Also note the focus of inflammatory cells (2) indicating that despite the chromic nature of this lesion, there is still ongoing active rejection and renal damage.
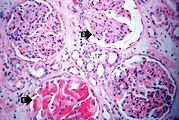
This high-power photomicrograph of glomeruli from this kidney demonstrates congestion (1), increased cellularity of glomeruli with mesangial expansion, and a glomerulus that is almost completely obliterated or sclerosed (2).

This is a photomicrograph of rejected kidney with a focus of cellular infiltrate (left) and a small artery with neointimal proliferation and stenosis (arrow).
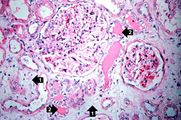
This is a photomicrograph of a glomerulus with a mild cellular infiltrate (left) and a small damaged glomerulus (right). There is extensive interstitial fibrosis (1), loss of renal tubules, and the remaining tubules contain protein (2) indicating severe damage.

This is a high-power photomicrograph of renal cortex with cellular infiltrate and few remaining renal tubules. The cellular infiltrate comprises macrophages, activated (large) lymphocytes and a few neutrophils and plasma cells.
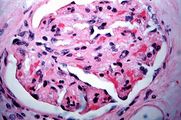
This is a high-power photomicrograph of a damaged glomerulus. Note the loss of normal capillary structure, the mesangial expansion and the infiltration of large mononuclear cells.

This is a high-power photomicrograph of a kidney from another case of chronic transplant rejection. In this case there is extensive damage to the kidney due to the chronic rejection (loss of tubules and glomerular lesions). In addition, this kidney was removed during an episode of acute rejection. The marked cellular infiltrate indicates acute rejection in a case of chronic transplant rejection.
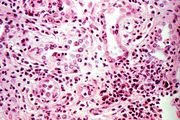
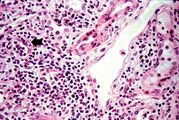
This is a higher-power photomicrograph of kidney from the previous image demonstrating the cellular infiltrate which is comprised of lymphocytes, macrophages, plasma cells and a few neutrophils.
Photomicrograph from another region of previous image. Note the cellular infiltrate around a small blood vessel (right) and neutrophils within renal tubules (arrow).












Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Assessment and Management of the Renal Transplant Patient
- eMedicine Medical Library: Renal Transplantation
- eMedicine Medical Library: Malignant Hypertension
- [www.merckmanuals.com/professional/cardiovascular_disorders/hypertension/hypertensive_emergencies.html Merck Manual: Hypertensive Emergencies]
- Merck Manual: Chronic Kidney Disease
- Merck Manual: Hemodialysis
- Merck Manual: Kidney Transplantation
Journal Articles[edit]
- Matas AJ. Impact of acute rejection on development of chronic rejection in pediatric renal transplant recipients. Pediatr Transplant 2000 May;4(2):92-9.
Images[edit]
Hypertension which has caused end-organ damage is termed malignant. Without proper treatment, these patients will usually die in less than 2 years. Blood pressures in patients with malignant hypertension are frequently 160/110 mm Hg or greater.
Renal failure is the severe reduction of renal function and often leads to reduced urinary output.
A normal BUN for this patient would be 10 to 20 mg/dL.
The normal creatinine level is 0.7 to 1.3 mg/dL.
A normal hematocrit for a male is 39 to 49%.
Azotemia is a condition of having excess nitrogen in the blood--a good indicator of reduced kidney function.
These tests are measures of kidney function. High levels mean low function.
A normal partial thromboplastin time is 28 to 37 seconds.
A normal kidney weighs 157 grams (range: 115 to 220 grams).
An infiltrate is an accumulation of cells in the lung parenchyma--this is a sign of pneumonia.