Difference between revisions of "IPLab:Lab 6:Amyloidosis"
Seung Park (talk | contribs) |
(→Images) |
||
| (9 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| − | This 46-year-old | + | This 46-year-old male with a long-standing history of rheumatoid arthritis was admitted for treatment of pneumonia. Subsequently, complications associated with lung abscesses, empyema, and septicemia led to the patient's death. |
| − | + | At autopsy the liver weighed 2600 grams. It was yellowish-tan in color and cut with difficulty (fibrosis?). No other pathological changes were noted except for pneumonia and lung abscesses. | |
| − | |||
== Images == | == Images == | ||
| Line 14: | Line 13: | ||
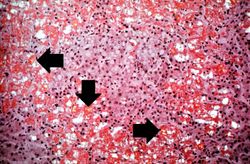
File:IPLab6Amyloid6.jpg|This is a low-power photomicrograph of liver tissue stained with Congo red (orange color in slide). Congo red reacts with amyloid and gives it an orange color (arrows). | File:IPLab6Amyloid6.jpg|This is a low-power photomicrograph of liver tissue stained with Congo red (orange color in slide). Congo red reacts with amyloid and gives it an orange color (arrows). | ||
File:IPLab6Amyloid7.jpg|This is a high-power view of liver tissue stained with Congo red. The orange amyloid material (arrows) is seen clearly between liver parenchymal cells. | File:IPLab6Amyloid7.jpg|This is a high-power view of liver tissue stained with Congo red. The orange amyloid material (arrows) is seen clearly between liver parenchymal cells. | ||
| − | File:IPLab6Amyloid8.jpg|This is a photomicrograph of Congo-red-stained liver tissue viewed with partially polarized light. Although not well demonstrated in this image, Congo-red-stained amyloid viewed through polarized light should give off a classic “apple green” birefringence (arrows). | + | File:IPLab6Amyloid8.jpg|This is a photomicrograph of Congo-red-stained liver tissue viewed with partially polarized light. Although not well demonstrated in this image, Congo-red-stained amyloid viewed through polarized light should give off a classic “apple green” birefringence (arrows). |
| + | File:IPLab6Amyloid8b.jpg|The amyloid in this Congo-red-stained liver tissue demonstrates the classic “apple green” birefringence when viewed through polarized light. | ||
File:IPLab6Amyloid9.jpg|This is a gross photograph of kidney from this case. Note the pale yellow material within the cortex (arrows). This is indicative of amyloid within the cortex and the glomeruli. Also note that there are multiple red spots in the cortex. These represent congested glomeruli due to the vascular compromise produced by the amyloid. | File:IPLab6Amyloid9.jpg|This is a gross photograph of kidney from this case. Note the pale yellow material within the cortex (arrows). This is indicative of amyloid within the cortex and the glomeruli. Also note that there are multiple red spots in the cortex. These represent congested glomeruli due to the vascular compromise produced by the amyloid. | ||
File:IPLab6Amyloid10.jpg|This photomicrograph of kidney demonstrates the amyloid deposits (arrows) within glomeruli. | File:IPLab6Amyloid10.jpg|This photomicrograph of kidney demonstrates the amyloid deposits (arrows) within glomeruli. | ||
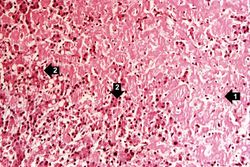
File:IPLab6Amyloid11.jpg|This photomicrograph of the tongue demonstrates extensive amyloid deposits (1) separating the skeletal muscle fibers of the tongue. In many cases the amyloid encircles the muscle fibers (2) and these muscle fibers are atrophied. | File:IPLab6Amyloid11.jpg|This photomicrograph of the tongue demonstrates extensive amyloid deposits (1) separating the skeletal muscle fibers of the tongue. In many cases the amyloid encircles the muscle fibers (2) and these muscle fibers are atrophied. | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Virtual Microscopy == | ||
| + | === Liver: Amyloid H&E === | ||
| + | <peir-vm>IPLab6Amyloid_HE</peir-vm> | ||
| + | |||
| + | === Liver: Amyloid Congo Red === | ||
| + | <peir-vm>IPLab6Amyloid_Congo_Red</peir-vm> | ||
| + | |||
| + | === Normal Liver H&E === | ||
| + | <peir-vm>UAB-Histology-00149</peir-vm> | ||
| + | |||
| + | == Study Questions == | ||
| + | * <spoiler text="What type of amyloid is this?">This is secondary amyloidosis because it is secondary to a chronic inflammatory condition. This would be an AA type of amyloid.</spoiler> | ||
| + | * <spoiler text="What is SAA protein, where is it produced, and what stimulates its production?">Serum amyloid-associated" protein is a protein produced by the liver when stimulated by interleukins 1 and 6.</spoiler> | ||
| + | * <spoiler text="What does hyaline mean?">Hyaline is a descriptive histologic term which refers to an alteration within cells or in the extracellular space which has a homogeneous, glassy, pink appearance in routine histologic sections stained with hematoxylin and eosin. | ||
| + | |||
| + | Amyloid is homogeneous, glassy, and pink in appearance; thus, we describe amyloid as having a hyaline appearance.</spoiler> | ||
| + | * <spoiler text="Is amyloid intracellular or extracellular?">Extracellular.</spoiler> | ||
| + | * <spoiler text="What other organs/tissues may be affected in patients with this type of amyloidosis?">Kidneys, heart, gastrointestinal tract, and tongue.</spoiler> | ||
| + | |||
| + | == Additional Resources == | ||
| + | === Reference === | ||
| + | * [http://emedicine.medscape.com/article/335414-overview eMedicine Medical Library: Amyloidosis] | ||
| + | * [http://emedicine.medscape.com/article/335559-overview eMedicine Medical Library: Amyloidosis, AA (Inflammatory)] | ||
| + | * [http://www.merckmanuals.com/professional/endocrine_and_metabolic_disorders/amyloidosis/amyloidosis.html Merck Manual: Amyloidosis] | ||
| + | |||
| + | === Journal Articles === | ||
| + | * Obici L, Merlini G. [http://www.ncbi.nlm.nih.gov/pubmed/22653707 AA amyloidosis: basic knowledge, unmet needs and future treatments]. ''Swiss Med Wkly'' 2012 May 31;142:w13580. | ||
| + | |||
| + | === Images === | ||
| + | * [{{SERVER}}/library/index.php?/tags/65-amyloidosis PEIR Digital Library: Amyloidosis Images] | ||
| + | * [http://library.med.utah.edu/WebPath/CINJHTML/CINJIDX.html#4 WebPath: Cellular Accumulations] | ||
| + | |||
| + | == Related IPLab Cases == | ||
| + | * [[IPLab:Lab 6:Multiple Myeloma|Lab 6: Multiple Myeloma with Amyloid]] | ||
| + | * [[IPLab:Lab 6:Senile Amyloidosis|Lab 6: Heart: Senile Amyloidosis]] | ||
| + | |||
{{IPLab 6}} | {{IPLab 6}} | ||
[[Category: IPLab:Lab 6]] | [[Category: IPLab:Lab 6]] | ||
Latest revision as of 00:22, 9 July 2020
Contents
Clinical Summary[edit]
This 46-year-old male with a long-standing history of rheumatoid arthritis was admitted for treatment of pneumonia. Subsequently, complications associated with lung abscesses, empyema, and septicemia led to the patient's death.
At autopsy the liver weighed 2600 grams. It was yellowish-tan in color and cut with difficulty (fibrosis?). No other pathological changes were noted except for pneumonia and lung abscesses.
Images[edit]
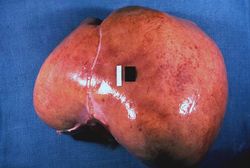
This is a gross picture of liver from this case. Note the pale, swollen appearance of this liver.
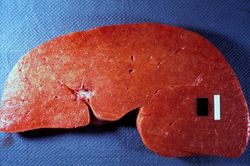
This is a gross picture of the cut surface of the liver from this case. The liver tissue is firm and has a waxy appearance--although this is difficult to appreciate in an image.
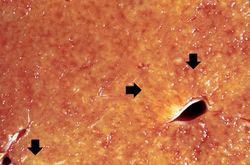
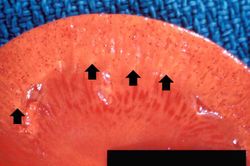
This is a closer view of the cut surface of this liver. The pale waxy material can be seen within the hepatic tissue (arrows).
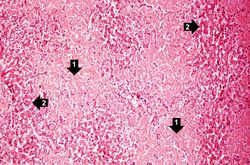
This is a low-power photomicrograph of liver tissue from this case. Note the eosinophilic hyaline material (1) present within and between the hepatic tissue (2). There is marked distortion of lobular architecture by the amyloid.
This is a higher-power photomicrograph showing the amyloid deposits (1) between hepatocytes (2).

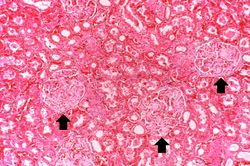
This is a low-power photomicrograph of liver tissue stained with Congo red (orange color in slide). Congo red reacts with amyloid and gives it an orange color (arrows).
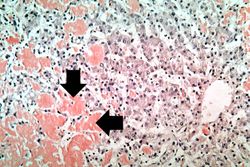
This is a high-power view of liver tissue stained with Congo red. The orange amyloid material (arrows) is seen clearly between liver parenchymal cells.
This is a photomicrograph of Congo-red-stained liver tissue viewed with partially polarized light. Although not well demonstrated in this image, Congo-red-stained amyloid viewed through polarized light should give off a classic “apple green” birefringence (arrows).
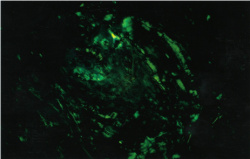
The amyloid in this Congo-red-stained liver tissue demonstrates the classic “apple green” birefringence when viewed through polarized light.
This is a gross photograph of kidney from this case. Note the pale yellow material within the cortex (arrows). This is indicative of amyloid within the cortex and the glomeruli. Also note that there are multiple red spots in the cortex. These represent congested glomeruli due to the vascular compromise produced by the amyloid.
This photomicrograph of kidney demonstrates the amyloid deposits (arrows) within glomeruli.
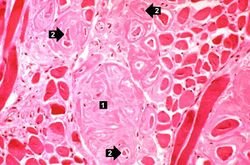
This photomicrograph of the tongue demonstrates extensive amyloid deposits (1) separating the skeletal muscle fibers of the tongue. In many cases the amyloid encircles the muscle fibers (2) and these muscle fibers are atrophied.












Virtual Microscopy[edit]
Liver: Amyloid H&E[edit]
Liver: Amyloid Congo Red[edit]
Normal Liver H&E[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Amyloidosis
- eMedicine Medical Library: Amyloidosis, AA (Inflammatory)
- Merck Manual: Amyloidosis
Journal Articles[edit]
- Obici L, Merlini G. AA amyloidosis: basic knowledge, unmet needs and future treatments. Swiss Med Wkly 2012 May 31;142:w13580.
Images[edit]
Related IPLab Cases[edit]
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.
An abscess is a collection of pus (white blood cells) within a cavity formed by disintegrated tissue.
A normal liver weighs 1650 grams (range: 1500 to 1800 grams).