Difference between revisions of "IPLab:Lab 13:Wilms Tumor"
Seung Park (talk | contribs) |
Seung Park (talk | contribs) |
||
| Line 18: | Line 18: | ||
File:IPLab13WT10.jpg|This high-power photomicrograph shows the differences in cell morphology between the blastema (1) and the fibroblast type cells (2). | File:IPLab13WT10.jpg|This high-power photomicrograph shows the differences in cell morphology between the blastema (1) and the fibroblast type cells (2). | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Study Questions == | ||
| + | * <spoiler text="What genetic factors predispose to the development of Wilms' tumors?">There are at least three known congenital malformations with defects in at least two chromosomal loci which predispose to Wilms' tumor. | ||
| + | |||
| + | The first group has the WAGR syndrome characterized by aniridia, genital anomalies, and mental retardation and a 33% chance of developing Wilms’ tumor. These patients have a gene defect proximal to chromosome 11 band p13 which is the Wilms’ tumor-associated gene, WT-1. | ||
| + | |||
| + | A second group of patients at risk for Wilms’ tumor have the Denys-Drash syndrome, which is characterized by gonadal dysgenesis (male pseudohermaphroditism) and nephropathy leading to renal failure. The majority of these patients develop Wilms’ tumors. The genetic abnormality in these children has also been mapped to chromosome 11, band p13. | ||
| + | |||
| + | The third group of patients at increased risk of developing Wilms’ tumor are those children with Beckwith-Wiedemann syndrome. This syndrome is characterized by enlargement of body organs, hemihypertrophy, renal medullary cysts, and abnormal large cells in adrenal cortex (adrenal cytomegaly). The genetic locus that is involved in these patients is in band p15.5 of chromosome 11 distal to the WT-1 locus. | ||
| + | |||
| + | The function of the second Wilms’ tumor gene (WT-2) is unknown. A few familial cases of Wilms’ tumors not associated with identifiable deletions or mutations involving either the WT-1 or the WT-2 gene suggest that there may be another locus that plays a role in some tumors.</spoiler> | ||
| + | * <spoiler text="What are the usual presenting signs with Wilms' tumor and what is the prognosis?">Children with Wilms’ tumors usually present with a large abdominal mass. | ||
| + | |||
| + | Hematuria, pain in the abdomen following some hemorrhagic incident, intestinal obstruction, and hypertension are other patterns of presentation. | ||
| + | |||
| + | With chemotherapy, radiotherapy, and surgery there is a 90% long-term survival rate.</spoiler> | ||
{{IPLab 13}} | {{IPLab 13}} | ||
[[Category: IPLab:Lab 13]] | [[Category: IPLab:Lab 13]] | ||
Revision as of 16:16, 21 August 2013
Clinical Summary[edit]
The mother of this three-year-old male noticed a large mass in his abdomen. There were no other complaints. Physical examination and x-rays--including an intravenous pyelogram (IVP)--showed a large right renal mass. At surgery, a 550-gram right kidney was removed. There was no lymph node involvement, no extrarenal mass, and no involvement of the other kidney. Lung and bone x-rays showed no metastases. However, microscopic study of the surgical specimen showed infiltration by the tumor (Grade II neoplasm) which had been difficult to separate from the duodenum. The child was placed on chemotherapy. Four months after the surgery to remove the tumor, a nodule was found in the lungs. The chemotherapy was resumed but the patient died four weeks later due to complications of Gram-negative sepsis.
Autopsy Findings[edit]
At autopsy there was a single tumor nodule in the lungs.
Images[edit]

This is a gross photograph of a bladder (1) to which are attached a normal kidney (2) and a kidney with Wilms' tumor (3). A large mass extends from the superior pole of the affected kidney. The renal capsule can be seen extending around this tumor.

This is a closer view of the kidney with Wilms' tumor (arrows).

This is a gross photograph of lung from this case demonstrating the metastatic tumor nodule (arrow).
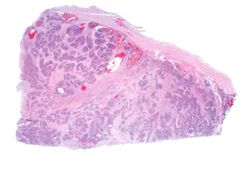
This lowest-power view shows the tumor itself; no tissue is present that can be readily identified as normal kidney. There does appear to be a capsule surrounding the tumor. Eosinophilic bands are seen surrounding basophilic islands of cells. These correspond to the two types of tissue in this tumor--the basophilic cellular component termed "blastema" can be distinguished from less cellular eosinophilic areas.
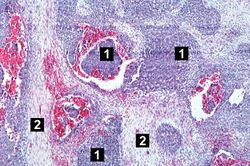
This low-power photomicrograph of tumor shows the two cell types making up this neoplasm. The basophilic cellular component termed "blastema" (1) can be distinguished from less cellular eosinophilic areas with fibroblast-like cells (2).

This medium-power photomicrograph of tumor shows again the two cell types making up this neoplasm. There are regions within the blastema where the cells form glands or "tubules" (arrows).
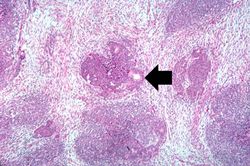
This is another medium-power photomicrograph of the tumor. It demonstrates again the two cell types making up this neoplasm. The glands or "tubules" within the blastema are better developed in this section (arrows).
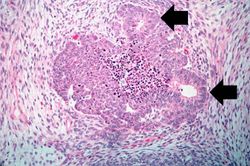
This is a high-power photomicrograph of "tubule" formation within the blastema (arrows).
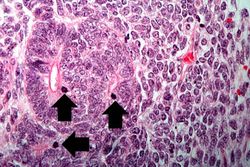
This high-power photomicrograph demonstrates tubule formation within the blastema. Note the numerous mitotic figures (arrows).
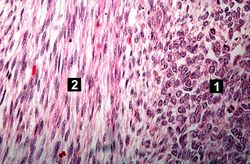
This high-power photomicrograph shows the differences in cell morphology between the blastema (1) and the fibroblast type cells (2).










Study Questions[edit]
| |||||
The patient is given an intravenous injection of contrast medium that rapidly enters the urine. Radiographs are then taken to show the passage of the contrast-containing urine through the pelvicaliceal system.
A normal kidney for a child this age should weigh 50 grams.
Gram-negative sepsis is a systemic inflammatory response caused by the presence of Gram-negative bacteria and their endotoxins in the blood. The microbes usually enter the bloodstream from an area of localized infection. Gram-negative sepsis is the leading cause of septic shock--hence, also known as "endotoxic shock." Septic shock is a syndrome of inflammatory responses which can lead to severe hypotension, multiple organ system failure, and death.
Renal failure is the severe reduction of renal function and often leads to reduced urinary output.
The normal fibrinogen level is 184 to 412 mg/dL.