IPLab:Lab 12:Radiation Changes
Contents
Clinical Summary
This 46-year-old white female was diagnosed with invasive squamous cell carcinoma of the cervix and subsequently received radiation therapy. Three years later the patient developed several episodes of small bowel obstruction which necessitated resection of a segment of ileum. She did well following surgery.
The surgical specimen consisted of a 13-cm segment of ileum having a luminal circumference of 5 cm. There was a full-thickness tear measuring 2.5 cm in the center of the specimen. On opening the bowel, the mucosa was ulcerated and showed a perforation.
Images

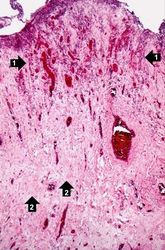
This is a low-power photomicrograph of the surgical specimen of the ileum. The normal ileum is to the left (1). The area of stricture consists of dense fibrous connective tissue (2) and there is loss or marked atrophy of the epithelium (3).

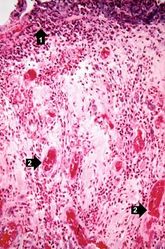
This is a higher-power photomicrograph of the surgical specimen of the ileum showing the transition from the normal epithelium (1) to the atrophied epithelium (2) in the area of radiation injury.
This is a higher-power photomicrograph showing the atrophied epithelium in the area of radiation injury. There are some epithelial cells deep within the mucosa (1). Note the dense fibrous connective tissue (2) within the wall of the ileum.
This is a high-power photomicrograph showing the atrophied epithelium in the area of radiation injury (1). Note the dense fibrous connective tissue within the wall of the ileum and the congested blood vessels (2).
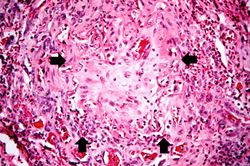
This is a high-power photomicrograph of the wall of the ileum showing a blood vessel that has suffered radiation-induced damage and is completely occluded (arrows).
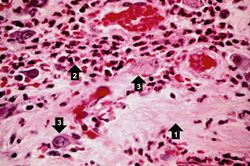
This high-power photomicrograph of the wall of the ileum shows areas of fibrosis (1), inflammatory cells (2), and abnormal pleomorphic cells (3) in the area of radiation injury. The abnormal morphology of these cells is radiation-induced. These cells are often difficult to distinguish from recurrent tumor cells.
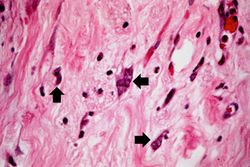
This high-power photomicrograph of the wall of the ileum shows more examples of pleomorphic cells (arrows) due to radiation injury.

This high-power photomicrograph of the wall of the ileum shows more examples of pleomorphic cells caused by radiation injury (arrows).








Virtual Microscopy
Study Questions
Additional Resources
Reference
- eMedicine Medical Library: Intestinal Radiation Injury
- eMedicine Medical Library: Radiation Therapy in Gynecology
- Merck Manual: Radiation Exposure and Contamination
Journal Articles
- Reis ED, Vine AJ, Heimann T. Radiation damage to the rectum and anus: pathophysiology, clinical features and surgical implications. Colorectal Dis 2002 Jan;4(1):2-12.
Images
| |||||