Difference between revisions of "IPLab:Lab 9:ARF"
Seung Park (talk | contribs) |
(→Clinical Summary) |
||
| (10 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
This 21-year-old black male with sickle cell anemia had recurrent attacks of acute rheumatic fever beginning at age 14. Mitral insufficiency and stenosis were present by age 16. On prophylactic antibiotics, the patient had no evidence of recurrence until three weeks before his final admission, when an upper respiratory infection developed. A few weeks later he developed acute migratory polyarthritis. This was associated with rapid deterioration of cardiac function and death. | This 21-year-old black male with sickle cell anemia had recurrent attacks of acute rheumatic fever beginning at age 14. Mitral insufficiency and stenosis were present by age 16. On prophylactic antibiotics, the patient had no evidence of recurrence until three weeks before his final admission, when an upper respiratory infection developed. A few weeks later he developed acute migratory polyarthritis. This was associated with rapid deterioration of cardiac function and death. | ||
| − | + | ||
| − | + | At autopsy, the heart was enlarged--weighing 675 grams--especially the left atrium. Both the aortic and mitral valves showed fibrosis as well as the fresh, tiny verrucae characteristic of acute rheumatic fever. | |
| − | At autopsy, the heart was enlarged--weighing 675 grams--especially the left atrium. Both the aortic and mitral valves showed fibrosis as well as the fresh, tiny verrucae characteristic of acute rheumatic fever. | ||
== Images == | == Images == | ||
| Line 14: | Line 13: | ||
File:IPLab9ARF6.jpg|This high-power photomicrograph of myocardium shows the cellular detail of another Aschoff body. In this case there appears to be a multinucleated Aschoff giant cell (arrow). | File:IPLab9ARF6.jpg|This high-power photomicrograph of myocardium shows the cellular detail of another Aschoff body. In this case there appears to be a multinucleated Aschoff giant cell (arrow). | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Virtual Microscopy == | ||
| + | <peir-vm>IPLab9ARF</peir-vm> | ||
| + | |||
| + | == Study Questions == | ||
| + | * <spoiler text="What is the etiology of rheumatic myocarditis?">Rheumatic fever is an acute, often recurrent, inflammatory disease that principally affects children following a pharyngeal (but not skin) infection with group A beta-hemolytic streptococci. Evidence strongly suggests that rheumatic fever is the result of an immune response to streptococcal antigens inciting either a cross-reaction to tissue antigens or a streptococcal-induced autoimmune reaction to normal tissue antigens.</spoiler> | ||
| + | * <spoiler text="Would it be possible to culture the causative agent from these lesions on the heart valves?">No. Rheumatic fever is an immune-mediated disease. No organisms can be cultured from the heart valves or from the Aschoff bodies.</spoiler> | ||
| + | * <spoiler text="Is this case an example of acute rheumatic fever?">Yes and no! | ||
| + | |||
| + | This patient has acute ramifications of rheumatic fever (acute valve lesions and Aschoff bodies) but there are also a number of old lesions in the heart suggesting that this patient has had numerous bouts of rheumatic fever over the course of many years.</spoiler> | ||
| + | |||
| + | == Additional Resources == | ||
| + | === Reference === | ||
| + | * [http://emedicine.medscape.com/article/236582-overview eMedicine Medical Library: Rheumatic Fever] | ||
| + | * [http://emedicine.medscape.com/article/808945-overview eMedicine Medical Library: Rheumatic Fever in Emergency Medicine] | ||
| + | * [http://emedicine.medscape.com/article/333103-overview eMedicine Medical Library: Acute Rheumatic Fever] | ||
| + | * [http://www.merckmanuals.com/professional/pediatrics/rheumatic_fever/rheumatic_fever.html Merck Manual: Rheumatic Fever] | ||
| + | |||
| + | === Journal Articles === | ||
| + | * American Heart Association Committee on Rheumatic Fever. [http://dx.doi.org/10.1161/CIR.0000000000000205 Revision of the Jones Criteria for the Diagnosis of Acute Rheumatic Fever in the Era of Doppler Echocardiography]. ''Circulation'' 2015 April 23; 131:1806-1818. | ||
| + | |||
| + | === Images === | ||
| + | * [{{SERVER}}/library/index.php?/tags/2153-streptococcus PEIR Digital Library: Streptococcus Images] | ||
| + | * [http://library.med.utah.edu/WebPath/CVHTML/CVIDX.html#8 Webpath: Myocarditis] | ||
{{IPLab 9}} | {{IPLab 9}} | ||
[[Category: IPLab:Lab 9]] | [[Category: IPLab:Lab 9]] | ||
Latest revision as of 21:44, 9 July 2020
Contents
Clinical Summary[edit]
This 21-year-old black male with sickle cell anemia had recurrent attacks of acute rheumatic fever beginning at age 14. Mitral insufficiency and stenosis were present by age 16. On prophylactic antibiotics, the patient had no evidence of recurrence until three weeks before his final admission, when an upper respiratory infection developed. A few weeks later he developed acute migratory polyarthritis. This was associated with rapid deterioration of cardiac function and death.
At autopsy, the heart was enlarged--weighing 675 grams--especially the left atrium. Both the aortic and mitral valves showed fibrosis as well as the fresh, tiny verrucae characteristic of acute rheumatic fever.
Images[edit]
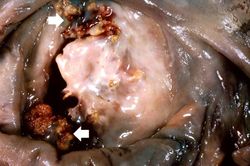
This is a gross photograph of mitral valve demonstrating marked thickening and fibrosis of the valve leaflet. There are also numerous foci of fibrinoid necrosis within the cusps and friable vegetations (verrucae) along the lines of closure (arrows). These irregular, warty projections are found at sites of erosion on the inflamed endocardial surface. The verrucae probably result from the precipitation of fibrin where the leaflets impinge on each other.

This is a low-power photomicrograph of heart tissue. Little can be seen at this magnification, except that the tissue looks relatively normal.
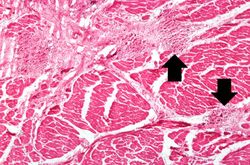
This is a higher-power photomicrograph of myocardium showing cellular accumulations--Aschoff bodies (arrows)--within the interstitium of the myocardium. These are found especially around blood vessels.
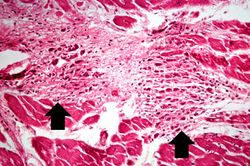
This is a higher-power photomicrograph of myocardium containing Aschoff bodies (arrows) within the interstitium.
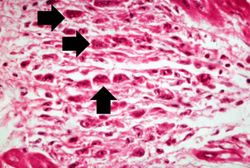
This high-power photomicrograph of myocardium shows the cellular detail of an Aschoff body. Aschoff bodies are foci of fibrinoid necrosis surrounded by lymphocytes, macrophages, an occasional plasma cell, and plump “activated” histiocytes called Anitschkow cells or Aschoff cells (arrows). These distinctive cells have abundant amphophilic cytoplasm and central round-to-ovoid nuclei in which the chromatin is disposed in a central, slender, wavy ribbon resembling a caterpillar (hence the designation “caterpillar cells”).

This high-power photomicrograph of myocardium shows the cellular detail of another Aschoff body. In this case there appears to be a multinucleated Aschoff giant cell (arrow).






Virtual Microscopy[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Rheumatic Fever
- eMedicine Medical Library: Rheumatic Fever in Emergency Medicine
- eMedicine Medical Library: Acute Rheumatic Fever
- Merck Manual: Rheumatic Fever
Journal Articles[edit]
- American Heart Association Committee on Rheumatic Fever. Revision of the Jones Criteria for the Diagnosis of Acute Rheumatic Fever in the Era of Doppler Echocardiography. Circulation 2015 April 23; 131:1806-1818.
Images[edit]
| |||||
Aortic insufficiency refers to the inability of the aortic valve to close properly, thus allowing regurgitation of blood into the left ventricle during diastole -- i.e., volume overload. Disease of the aortic valve leaflets is a common cause of insufficiency.
A normal heart weighs 300 grams (range: 270 to 360 grams).
Friable material is easily crumbled.
Autoimmune disorders involve an immune response directed at the host's own cells.