Difference between revisions of "IPLab:Lab 5:Nodular Intercapillary Glomerulosclerosis"
(→Journal Articles) |
(→Images) |
||
| (3 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| − | This 57-year-old white male with a 25-year history of Type | + | This 57-year-old white male with a 25-year history of Type 1 diabetes mellitus developed an acute myocardial infarction followed by cerebral infarction, pulmonary dysfunction, and renal failure. There was a history of hypertension, proteinuria, and elevations in BUN and creatinine. He subsequently died of multisystem failure. |
| − | + | The autopsy showed concentric left ventricular hypertrophy, an acute myocardial infarction, and a right cerebral infarction. The pancreas showed amyloidosis of the islets. There was extensive atherosclerosis and arteriolosclerosis. The kidneys were large, weighing 220 and 240 grams respectively, and had a rough surface, a few cortical scars, and blurring of the corticomedullary junctions. | |
| − | The autopsy showed | ||
== Images == | == Images == | ||
<gallery heights="250px" widths="250px"> | <gallery heights="250px" widths="250px"> | ||
File:IPLab5DM1.jpg|This is a gross photograph of the kidneys from this case. Note that there are multiple shrunken regions (old infarcts) (arrows) and the kidneys have a rough granular appearance on the surface, which is caused by multiple small infarcts of small vessels throughout the cortex. | File:IPLab5DM1.jpg|This is a gross photograph of the kidneys from this case. Note that there are multiple shrunken regions (old infarcts) (arrows) and the kidneys have a rough granular appearance on the surface, which is caused by multiple small infarcts of small vessels throughout the cortex. | ||
| − | File: | + | File:IPLab5DM2b.jpg|This is a low-power photomicrograph of the kidney from this patient. The section extends from cortex (1) to the medulla (2). |
| − | File: | + | File:IPLab5DM3b.jpg|This is a higher-power photomicrograph of the cortical region. In this region there is ischemic obsolescence of glomeruli and one glomerulus with nodular glomerulosclerosis (1). Also note the thickened walls of the blood vessels (2). |
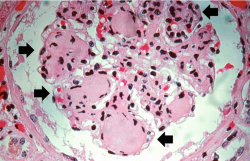
| − | File: | + | File:IPLab5DM4b.jpg|This is a high-power photomicrograph of two glomeruli with intercapillary glomerulosclerosis (arrows). |
| − | File: | + | File:IPLab5DM5b.jpg|This is a photomicrograph of a glomerulus with nodular glomerulosclerosis (1). Also note the intertubular fibrosis and the changes in the blood vessels (2). |
| − | File: | + | File:IPLab5DM6b.JPG|This is a higher-power photomicrograph of a glomerulus with nodular glomerulosclerosis (arrows). These are the classic Kimmelstiel-Wilson lesions ("K-W lesions") seen in diabetics with nodular glomerulosclerosis. |
| − | File: | + | File:IPLab5DM7b.jpg|This is a photomicrograph of kidney with a focal exudative lesion in a glomerulus (arrow) and sclerosis, interstitial fibrosis, and congestion. |
</gallery> | </gallery> | ||
Latest revision as of 20:03, 8 July 2020
Contents
Clinical Summary[edit]
This 57-year-old white male with a 25-year history of Type 1 diabetes mellitus developed an acute myocardial infarction followed by cerebral infarction, pulmonary dysfunction, and renal failure. There was a history of hypertension, proteinuria, and elevations in BUN and creatinine. He subsequently died of multisystem failure.
The autopsy showed concentric left ventricular hypertrophy, an acute myocardial infarction, and a right cerebral infarction. The pancreas showed amyloidosis of the islets. There was extensive atherosclerosis and arteriolosclerosis. The kidneys were large, weighing 220 and 240 grams respectively, and had a rough surface, a few cortical scars, and blurring of the corticomedullary junctions.
Images[edit]

This is a gross photograph of the kidneys from this case. Note that there are multiple shrunken regions (old infarcts) (arrows) and the kidneys have a rough granular appearance on the surface, which is caused by multiple small infarcts of small vessels throughout the cortex.
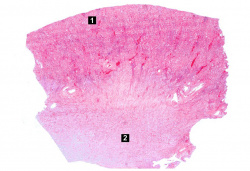
This is a low-power photomicrograph of the kidney from this patient. The section extends from cortex (1) to the medulla (2).
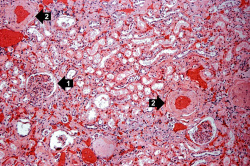
This is a higher-power photomicrograph of the cortical region. In this region there is ischemic obsolescence of glomeruli and one glomerulus with nodular glomerulosclerosis (1). Also note the thickened walls of the blood vessels (2).
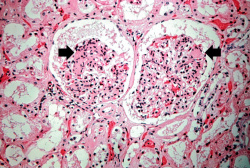
This is a high-power photomicrograph of two glomeruli with intercapillary glomerulosclerosis (arrows).
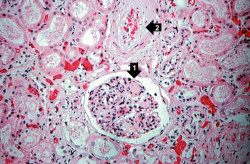
This is a photomicrograph of a glomerulus with nodular glomerulosclerosis (1). Also note the intertubular fibrosis and the changes in the blood vessels (2).
This is a higher-power photomicrograph of a glomerulus with nodular glomerulosclerosis (arrows). These are the classic Kimmelstiel-Wilson lesions ("K-W lesions") seen in diabetics with nodular glomerulosclerosis.
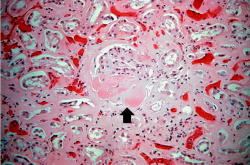
This is a photomicrograph of kidney with a focal exudative lesion in a glomerulus (arrow) and sclerosis, interstitial fibrosis, and congestion.







Virtual Microscopy[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Type 1 Diabetes Mellitus
- eMedicine Medical Library: Type 2 Diabetes Mellitus
- Merck Manual: Diabetes Mellitus (DM)
Journal Articles[edit]
- Herzenberg AM, Holden JK, Singh S, Magil AB. Idiopathic nodular glomerulosclerosis. Am J Kidney Dis 1999 Sep;34(3):560-4.
- Vinik AI. Diabetic Sensory and Motor Neuropathy. N Engl J Med" 2016 April 14; 374:1455-1464.
- Kamel KS and Halperin ML. Acid–Base Problems in Diabetic Ketoacidosis. N Engl J Med" 2015 Feb 5;372:546-554.
Images[edit]
- PEIR Digital Library: Diabetic Glomerulosclerosis Images
- WebPath: Interstitial Diseases of the Kidney
Related IPLab Cases[edit]
| |||||
Myocardial infarction is necrosis of myocardial tissue which occurs as a result of a deprivation of blood supply, and thus oxygen, to the heart tissue. Blockage of blood supply to the myocardium is caused by occlusion of a coronary artery.
Renal failure is the severe reduction of renal function and often leads to reduced urinary output.
Protein in the urine is indicative of glomerular dysfunction.
These tests are measures of kidney function. High levels mean low function.
A normal kidney weighs 157 grams (range: 115 to 220 grams).
Nodular hyperplasia of the prostate--characterized by large discrete prostatic nodules--is a common disorder in men over 50 years of age. The nodules cause the prostate to be enlarged and to have an increased weight. The human prostate is surrounded by a restrictive capsule. These nodules cause increased pressure within the capsule which leads to constriction of the urethra as it passes through the prostate. Urethral constriction leads to retention of urine.