Difference between revisions of "IPLab:Lab 5:Gaucher Disease"
Seung Park (talk | contribs) |
Seung Park (talk | contribs) |
||
| Line 16: | Line 16: | ||
File:IPLab5Gaucher8.jpg|This is a higher-power photomicrograph of the spleen from this case. At this higher power individual cells can be better appreciated and the fibrillar nature of the eosinophilic cytoplasmic material can be seen. | File:IPLab5Gaucher8.jpg|This is a higher-power photomicrograph of the spleen from this case. At this higher power individual cells can be better appreciated and the fibrillar nature of the eosinophilic cytoplasmic material can be seen. | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Study Questions == | ||
| + | * <spoiler text="What is the inheritance pattern of the various forms of Gaucher disease and what gene is involved?">Gaucher disease has an autosomal recessive inheritance pattern. There is a mutation of the glucocerebrosidase gene on chromosome 1q21.</spoiler> | ||
| + | * <spoiler text="What are the 3 clinical presentations that have been described for Gaucher disease?">Type I makes up 99% of the reported cases of Gaucher disease. This is termed the chronic non-neuronopathic form of Gaucher disease. In type I the build up of glucocerebrosides is only observed in phagocytic cells throughout the body, especially in the spleen, liver, and skeletal muscles. There is no brain involvement. Type I is seen primarily in Jews of European decent. Patients with this form of Gaucher disease have reduced but detectable levels of glucocerebrosidase activity. Life span is slightly shortened in these patients. | ||
| + | |||
| + | Type II is termed the infantile acute neuronopathic form of Gaucher disease. Though hepatosplenomegaly is also seen in this form of Gaucher disease, there is a progressive central nervous system involvement leading to death at an early age. There is no detectable glucocerebrosidase activity in the tissues and there is no predilection for Jews. | ||
| + | |||
| + | The third pattern, type III, is usually somewhat intermediate between types I and II. These patients are usually juveniles and have systemic involvement like in type I but they have progressive central nervous system disease that usually begins in the second or third decade of life.</spoiler> | ||
| + | * <spoiler text="What type of Gaucher disease did this patient likely have?">This was an adult who had pancytopenia and aseptic necrosis of bone. This is consistent with type I. In type I symptoms and signs first appear in adult life and are related to splenomegaly or to bone involvement by Gaucher cells. These patients have pancytopenia or thrombocytopenia secondary to hypersplenism and pathologic fractures and bone pain due to expansion of the marrow space by Gaucher cells.</spoiler> | ||
{{IPLab 5}} | {{IPLab 5}} | ||
[[Category: IPLab:Lab 5]] | [[Category: IPLab:Lab 5]] | ||
Revision as of 15:13, 21 August 2013
Clinical Summary =[edit]
This 23-year-old black female delivered a stillborn infant by Caesarean section, following which she experienced excessive uterine bleeding including the passage of blood clots. Further study revealed an enlarged spleen and thrombocytopenia (platelet count 58,000). A splenectomy was performed with an uneventful postoperative course other than persistent pain in her right leg (the right hip had been fractured 2 years earlier). Subsequently she developed aseptic necrosis of the left femoral head requiring a prosthetic replacement. Microscopic evaluation of the bone removed at the time of surgery revealed Gaucher cells in the marrow space.
Autopsy Findings[edit]
The surgical specimen was a 935-gram spleen. Its surface was pale with an area of bluish discoloration. The cut surface revealed the same pale appearance.
Images[edit]

This is a gross photograph of spleen from this case. The spleen is enlarged and the surface is finely granular.

This is a cut section of spleen from this case. Again note the fine granular appearance to the tissue.
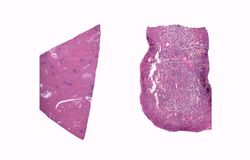
This is a low-power photomicrograph of normal spleen (left) and the spleen from this case (right). The loose appearance of the tissue in the Gaucher spleen is due to artifactual loss of tissue during histologic processing.
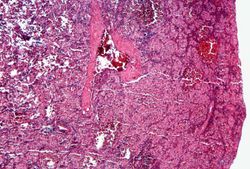
This is a photomicrograph of the spleen from this case. There is very little if any white pulp evident in this section.
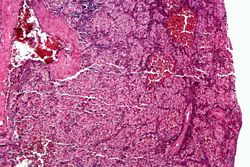
This is a higher-power photomicrograph of the spleen from this case. Again there is no white pulp and the red pulp is filled with large eosinophilic cells.
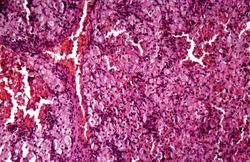
This is another high-power photomicrograph of the spleen from this case. At this power it is easier to see the large eosinophilic cells.
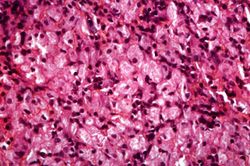
This is another high-power photomicrograph of the spleen from this case. At this high power individual cells can be better appreciated.
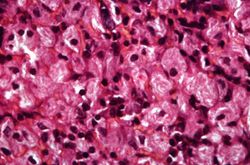
This is a higher-power photomicrograph of the spleen from this case. At this higher power individual cells can be better appreciated and the fibrillar nature of the eosinophilic cytoplasmic material can be seen.








Study Questions[edit]
| |||||
The normal platelet count is 150,000 to 400,000/mm³.
Trauma (from fracture or surgery) is one cause of asceptic (or avascular) necrosis of bone, which is defined as the death of bone and bone marrow in the abscence of an infectious agent.