Difference between revisions of "IPLab:Lab 5:α1 Antitrypsin Deficiency"
Seung Park (talk | contribs) (→Images) |
(→Images) |
||
| (3 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| − | This 68-year-old white female was afflicted with severe emphysema due to | + | This 68-year-old white female was afflicted with severe emphysema due to alpha 1-antitrypsin deficiency. She had a 10 pack-year history of cigarette smoking but she had quit smoking 30 years ago. She elected to undergo lung volume reduction surgery to reduce complications of her emphysema. Post-operatively, she was ventilator dependent and her liver function declined. Further studies revealed hepatic cirrhosis. Her pulmonary function continued to decline and she died 26 days after her surgery. |
| − | + | At autopsy there were severe emphysematous changes in all lung lobes and there was massive hemorrhage throughout the lungs. The liver weighed 860 grams and there was micronodular cirrhosis. | |
| − | |||
== Images == | == Images == | ||
<gallery heights="250px" widths="250px"> | <gallery heights="250px" widths="250px"> | ||
| − | File: | + | File:IPLab5Antitrypsin1b.jpg|This is a gross photograph of the lungs from this case. The rough friable material on the surface of the lung (arrows) is fibrinous exudate and fibrous tissue. This reaction on the surface of the lung is due to the recent surgery. The emphysematous changes are not easily appreciated in this photograph. |
| − | File: | + | File:IPLab5Antitrypsin2b.jpg|This is a gross photograph of the cut sections of lung from this case. The lung parenchyma is markedly hemorrhagic and consolidated. Again the hemorrhage makes it difficult to appreciate the emphysematous changes. |
| − | File: | + | File:IPLab5Antitrypsin3b.jpg|This is a gross photograph of the bronchi and lungs. Note the hemorrhage in the bronchi and in the lung parenchyma. |
| − | File: | + | File:IPLab5Antitrypsin4b.jpg|This low-power photomicrograph demonstrates the hemorrhage present throughout the lung. Note also the large air spaces; even though they are filled with blood, the emphysematous enlargement of the spaces is appreciable. |
| − | File: | + | File:IPLab5Antitrypsin5b.jpg|This is a low-power photomicrograph from an area of the lung without significant hemorrhage. The enlarged, emphysematous air spaces are easily appreciated. |
File:IPLab5Antitrypsin6.jpg|This is a gross photograph of the liver from this case. The capsule is somewhat thickened and the surface is slightly roughened, though it is difficult to appreciate the nodularity of the liver. | File:IPLab5Antitrypsin6.jpg|This is a gross photograph of the liver from this case. The capsule is somewhat thickened and the surface is slightly roughened, though it is difficult to appreciate the nodularity of the liver. | ||
File:IPLab5Antitrypsin7.jpg|This is a gross photograph of the cut section of liver from this case. In this view the liver looks smaller than normal and there is a definite micronodular appearance. | File:IPLab5Antitrypsin7.jpg|This is a gross photograph of the cut section of liver from this case. In this view the liver looks smaller than normal and there is a definite micronodular appearance. | ||
| − | File: | + | File:IPLab5Antitrypsin8b.jpg|This is a closer view of the cut section of liver from this case. There is a definite micronodular pattern to the liver parenchyma. |
File:IPLab5Antitrypsin9.jpg|This is a low-power photomicrograph of an H&E-stained section of liver. There are increased numbers of inflammatory cells in the periportal region (arrow) and the central vein areas are pale. | File:IPLab5Antitrypsin9.jpg|This is a low-power photomicrograph of an H&E-stained section of liver. There are increased numbers of inflammatory cells in the periportal region (arrow) and the central vein areas are pale. | ||
File:IPLab5Antitrypsin10.jpg|This is a low-power photomicrograph of a trichrome-stained section of liver. There is bridging fibrosis (blue material) between portal regions. | File:IPLab5Antitrypsin10.jpg|This is a low-power photomicrograph of a trichrome-stained section of liver. There is bridging fibrosis (blue material) between portal regions. | ||
Latest revision as of 19:45, 8 July 2020
Contents
Clinical Summary[edit]
This 68-year-old white female was afflicted with severe emphysema due to alpha 1-antitrypsin deficiency. She had a 10 pack-year history of cigarette smoking but she had quit smoking 30 years ago. She elected to undergo lung volume reduction surgery to reduce complications of her emphysema. Post-operatively, she was ventilator dependent and her liver function declined. Further studies revealed hepatic cirrhosis. Her pulmonary function continued to decline and she died 26 days after her surgery.
At autopsy there were severe emphysematous changes in all lung lobes and there was massive hemorrhage throughout the lungs. The liver weighed 860 grams and there was micronodular cirrhosis.
Images[edit]
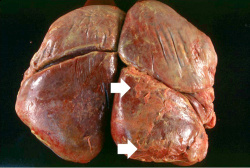
This is a gross photograph of the lungs from this case. The rough friable material on the surface of the lung (arrows) is fibrinous exudate and fibrous tissue. This reaction on the surface of the lung is due to the recent surgery. The emphysematous changes are not easily appreciated in this photograph.
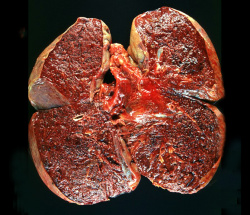
This is a gross photograph of the cut sections of lung from this case. The lung parenchyma is markedly hemorrhagic and consolidated. Again the hemorrhage makes it difficult to appreciate the emphysematous changes.
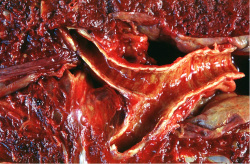
This is a gross photograph of the bronchi and lungs. Note the hemorrhage in the bronchi and in the lung parenchyma.
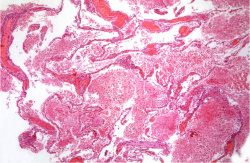
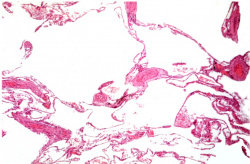
This low-power photomicrograph demonstrates the hemorrhage present throughout the lung. Note also the large air spaces; even though they are filled with blood, the emphysematous enlargement of the spaces is appreciable.
This is a low-power photomicrograph from an area of the lung without significant hemorrhage. The enlarged, emphysematous air spaces are easily appreciated.

This is a gross photograph of the liver from this case. The capsule is somewhat thickened and the surface is slightly roughened, though it is difficult to appreciate the nodularity of the liver.

This is a gross photograph of the cut section of liver from this case. In this view the liver looks smaller than normal and there is a definite micronodular appearance.
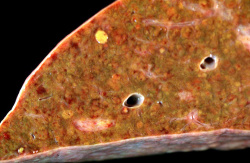
This is a closer view of the cut section of liver from this case. There is a definite micronodular pattern to the liver parenchyma.
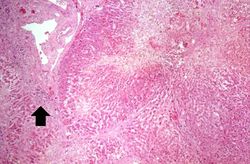
This is a low-power photomicrograph of an H&E-stained section of liver. There are increased numbers of inflammatory cells in the periportal region (arrow) and the central vein areas are pale.
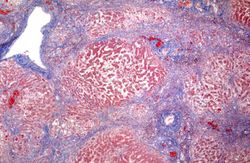
This is a low-power photomicrograph of a trichrome-stained section of liver. There is bridging fibrosis (blue material) between portal regions.
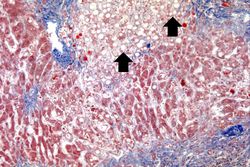
This is a higher-power photomicrograph of a trichrome-stained section of liver. This section demonstrates the fibrosis (blue material) and the fatty change (arrows).
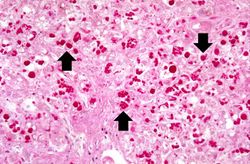
This is a high-power photomicrograph of liver stained with periodic-acid Schiff's (PAS) stain. This demonstrates the PAS-positive granules of defective α1-antitrypsin that accumulate in the Golgi of hepatocytes (arrows).












Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: α1-Antitrypsin Deficiency
- eMedicine Medical Library: Emphysema
- eMedicine Medical Library: COPD and Emphysema
- Merck Manual: α1-Antitrypsin Deficiency
Journal Articles[edit]
- Perlmutter DH. Liver injury in α1-antitrypsin deficiency. Clin Liver Dis 2000 May;4(2):387-408, vi.
Images[edit]
- PEIR Digital Library: Emphysema Images
- PEIR Digital Library: α1-Antitrypsin Deficiency Images
- WebPath: Emphysema
Related IPLab Cases[edit]
- Lab 2: Liver: Fatty Change and Cirrhosis
- Lab 10: Lung: Cryptococcosis
- Lab 12: Lung: Chronic Obstructive Pulmonary Disease
| |||||
Pulmonary emphysema is a condition in which the air spaces distal to the terminal bronchioles are permanently increased in size due to either destruction of the wall or alveolar dilatation.
A pack-year denotes smoking one pack of cigarettes per day for one year.
Cirrhosis is a liver disease characterized by necrosis, fibrosis, loss of normal liver architecture, and hyperplastic nodules.
A normal partial thromboplastin time is 28 to 37 seconds.
Friable material is easily crumbled.
Consolidation is the filling of lung air spaces with exudate--this is a sign of pneumonia.