Difference between revisions of "IPLab:Lab 2:Hyperplasia"
(→Images) |
|||
| (7 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| − | This 87-year-old man | + | This 87-year-old man has had a three year history of difficulty in starting his urine stream. He was seen several times in the emergency room for acute urinary retention and dysuria. On several occasions, significant numbers of white blood cells and bacteria (suggestive of acute cystitis) were noted in the patient's urine specimen. |
| − | + | ||
Terminally, the patient developed fever, confusion that progressed to coma, convulsions, and shock. At the time of his death, the patient's major clinical problem was Gram-negative sepsis secondary to a urinary tract infection. | Terminally, the patient developed fever, confusion that progressed to coma, convulsions, and shock. At the time of his death, the patient's major clinical problem was Gram-negative sepsis secondary to a urinary tract infection. | ||
| − | + | At autopsy the prostate gland was grossly enlarged (6.5 x 4.8 x 3.2 cm) and weighed 75 grams. The prostate gland was nodular but the nodules were confined within the prostatic capsule. | |
| − | At autopsy the prostate gland was grossly enlarged (6.5 x 4.8 x 3.2 cm) and weighed 75 grams. The prostate gland was nodular but the nodules were confined within the prostatic capsule. | ||
== Images == | == Images == | ||
| Line 13: | Line 12: | ||
File:IPLab2Hyperplasia3.jpg|This is a low-power photomicrograph showing hyperplastic prostate on the left (1) and normal prostate on the right (2). At this power, dilated glands are visible in the section of hyperplastic prostate. | File:IPLab2Hyperplasia3.jpg|This is a low-power photomicrograph showing hyperplastic prostate on the left (1) and normal prostate on the right (2). At this power, dilated glands are visible in the section of hyperplastic prostate. | ||
File:IPLab2Hyperplasia4.jpg|The dilated glands (arrows) make up the major portion of the prostate tissue and there is compression of the stroma. | File:IPLab2Hyperplasia4.jpg|The dilated glands (arrows) make up the major portion of the prostate tissue and there is compression of the stroma. | ||
| − | |||
File:IPLab2Hyperplasia6.jpg|Cystic dilatation of glands is present in this photomicrograph. Notice the accumulation of secretory material inside the glands (arrows) and compression (thinning) of the lining epithelium. | File:IPLab2Hyperplasia6.jpg|Cystic dilatation of glands is present in this photomicrograph. Notice the accumulation of secretory material inside the glands (arrows) and compression (thinning) of the lining epithelium. | ||
File:IPLab2Hyperplasia7.jpg|A higher-power view shows the papillary folds (arrows) produced by the hyperplastic epithelium projecting into the lumen of the gland. While these papillary folds project into the lumen of the gland, there is no extension through the glandular basement membrane into the gland's stroma. | File:IPLab2Hyperplasia7.jpg|A higher-power view shows the papillary folds (arrows) produced by the hyperplastic epithelium projecting into the lumen of the gland. While these papillary folds project into the lumen of the gland, there is no extension through the glandular basement membrane into the gland's stroma. | ||
| Line 19: | Line 17: | ||
File:IPLab2Hyperplasia9.jpg|This kidney was removed from another autopsy patient who had prostatic hyperplasia resulting in marked urinary retention and back-flow of urine from the bladder into the ureters and renal pelvis. The increased pressure inside the renal pelvis resulted in dilation of the renal pelvis (1) and pressure atrophy of the cortex (2). This change in the kidney is called hydronephrosis. | File:IPLab2Hyperplasia9.jpg|This kidney was removed from another autopsy patient who had prostatic hyperplasia resulting in marked urinary retention and back-flow of urine from the bladder into the ureters and renal pelvis. The increased pressure inside the renal pelvis resulted in dilation of the renal pelvis (1) and pressure atrophy of the cortex (2). This change in the kidney is called hydronephrosis. | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Virtual Microscopy == | ||
| + | === Prostatic Hyperplasia === | ||
| + | <peir-vm>IPLab2Hyperplasia</peir-vm> | ||
| + | |||
| + | === Normal Prostate === | ||
| + | <peir-vm>IPLab2Hyperplasia_normal_Prostate</peir-vm> | ||
== Study Questions == | == Study Questions == | ||
| Line 26: | Line 31: | ||
* <spoiler text="What is the age-specific incidence of nodular hyperplasia in males?">The incidence of nodular hyperplasia is: | * <spoiler text="What is the age-specific incidence of nodular hyperplasia in males?">The incidence of nodular hyperplasia is: | ||
| − | 20% in men 40 years of age | + | * 20% in men 40 years of age |
| − | 30% in men 50 years of age | + | * 30% in men 50 years of age |
| − | 70% in men 60 years of age | + | * 70% in men 60 years of age |
| − | 90% in men 70 years of age</spoiler> | + | * 90% in men 70 years of age</spoiler> |
* <spoiler text="Does nodular hyperplasia predispose to adenocarcinoma?">No.</spoiler> | * <spoiler text="Does nodular hyperplasia predispose to adenocarcinoma?">No.</spoiler> | ||
* <spoiler text="What other conditions can be associated with or result from nodular hyperplasia of the prostate?">Urinary retention, cystitis, bladder distention, hypertrophy, trabeculation, diverticulum formation, renal infections, and hydronephrosis.</spoiler> | * <spoiler text="What other conditions can be associated with or result from nodular hyperplasia of the prostate?">Urinary retention, cystitis, bladder distention, hypertrophy, trabeculation, diverticulum formation, renal infections, and hydronephrosis.</spoiler> | ||
| + | |||
| + | == Additional Resources == | ||
| + | |||
| + | === Reference === | ||
| + | * [http://emedicine.medscape.com/article/231574-overview eMedicine Medical Library: Urinary Tract Infection in Males] | ||
| + | * [http://www.merckmanuals.com/professional/genitourinary_disorders/benign_prostate_disease/benign_prostatic_hyperplasia_bph.html Merck Manual: Benign Prostatic Disease] | ||
| + | |||
| + | === Journal Articles === | ||
| + | * Wang TJ, Slawin KM, Rittenhouse HG, Millar LS, Mikolajczyk SD. [http://www.ncbi.nlm.nih.gov/pubmed/10866804 Benign prostatic hyperplasia-associated prostate-specific antigen (BPSA) shows unique immunoreactivity with anti-PSA monoclonal antibodies]. ''Eur J Biochem'' 2000 Jul;267(13):4040-5. | ||
| + | |||
| + | === Images === | ||
| + | * [{{SERVER}}/library/index.php?/tags/145-male_reproductive/146-prostate/147-hyperplasia PEIR Digital Library: Prostatic Hyperplasia Images] | ||
| + | * [http://library.med.utah.edu/WebPath/MALEHTML/MALEIDX.html WebPath: Male Genital Pathology] | ||
{{IPLab 2}} | {{IPLab 2}} | ||
[[Category: IPLab:Lab 2]] | [[Category: IPLab:Lab 2]] | ||
Latest revision as of 20:05, 19 June 2020
Contents
Clinical Summary[edit]
This 87-year-old man has had a three year history of difficulty in starting his urine stream. He was seen several times in the emergency room for acute urinary retention and dysuria. On several occasions, significant numbers of white blood cells and bacteria (suggestive of acute cystitis) were noted in the patient's urine specimen.
Terminally, the patient developed fever, confusion that progressed to coma, convulsions, and shock. At the time of his death, the patient's major clinical problem was Gram-negative sepsis secondary to a urinary tract infection.
At autopsy the prostate gland was grossly enlarged (6.5 x 4.8 x 3.2 cm) and weighed 75 grams. The prostate gland was nodular but the nodules were confined within the prostatic capsule.
Images[edit]
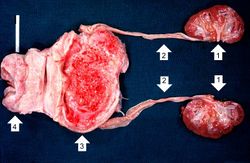
This photograph shows the autopsy specimen from this patient. Included are kidneys (1), ureters (2), bladder (3) (which has been opened), and enlarged prostate (4). Note that the bladder mucosa has multiple trabeculae and the bladder mucosa is hyperemic. Also note that the ureters are dilated.

This is a close-up of the prostate from this same patient. Note the nodularity of the tissue (1) and the enlargement of the gland. Enlargement of the prostate leads to compression of the urethra as it passes through (2) the gland.
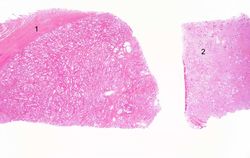
This is a low-power photomicrograph showing hyperplastic prostate on the left (1) and normal prostate on the right (2). At this power, dilated glands are visible in the section of hyperplastic prostate.
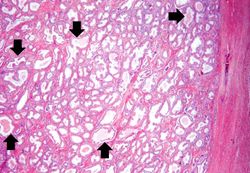
The dilated glands (arrows) make up the major portion of the prostate tissue and there is compression of the stroma.

Cystic dilatation of glands is present in this photomicrograph. Notice the accumulation of secretory material inside the glands (arrows) and compression (thinning) of the lining epithelium.
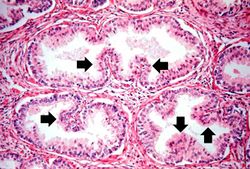
A higher-power view shows the papillary folds (arrows) produced by the hyperplastic epithelium projecting into the lumen of the gland. While these papillary folds project into the lumen of the gland, there is no extension through the glandular basement membrane into the gland's stroma.

This is a higher-power photomicrograph of papillary folds of hyperplastic epithelium (arrows).

This kidney was removed from another autopsy patient who had prostatic hyperplasia resulting in marked urinary retention and back-flow of urine from the bladder into the ureters and renal pelvis. The increased pressure inside the renal pelvis resulted in dilation of the renal pelvis (1) and pressure atrophy of the cortex (2). This change in the kidney is called hydronephrosis.








Virtual Microscopy[edit]
Prostatic Hyperplasia[edit]
Normal Prostate[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
Journal Articles[edit]
- Wang TJ, Slawin KM, Rittenhouse HG, Millar LS, Mikolajczyk SD. Benign prostatic hyperplasia-associated prostate-specific antigen (BPSA) shows unique immunoreactivity with anti-PSA monoclonal antibodies. Eur J Biochem 2000 Jul;267(13):4040-5.
Images[edit]
| |||||
"Urinary retention" is the inability to fully empty the bladder during urination.
"Dysuria" is the experience of pain upon urination.
"Cystitis" refers to an infection of the urinary bladder.
Gram-negative sepsis is a systemic inflammatory response caused by the presence of Gram-negative bacteria and their endotoxins in the blood. The microbes usually enter the bloodstream from an area of localized infection. Gram-negative sepsis is the leading cause of septic shock--hence, also known as "endotoxic shock." Septic shock is a syndrome of inflammatory responses which can lead to severe hypotension, multiple organ system failure, and death.
The dimensions of a normal prostate are 3.6 x 2.8 x 1.9 cm. So this prostate is enlarged.
Normally, a prostate in an 80 year old man should weigh about 40 grams.
Nodular hyperplasia of the prostate--characterized by large discrete prostatic nodules--is a common disorder in men over 50 years of age. The nodules cause the prostate to be enlarged and to have an increased weight. The human prostate is surrounded by a restrictive capsule. These nodules cause increased pressure within the capsule which leads to constriction of the urethra as it passes through the prostate. Urethral constriction leads to retention of urine.
Prostate carcinomas spread through the capsule at an early stage, thus these nodules are more likely not to be cancer.
Hydronephrosis is dilation of the renal pelvis and atrophy of the cortex due to increase pressure from retained urine.
The normal fibrinogen level is 184 to 412 mg/dL.