Difference between revisions of "IPLab:Lab 2:Atrophy"
Seung Park (talk | contribs) |
|||
| Line 16: | Line 16: | ||
File:IPLab2Atrophy9.jpg|The two kidneys in this slide are from the same patient. One kidney (1) is relatively normal, although increased in size due to compensatory hypertrophy. The other kidney (2) is very small with only rudimentary nodules of renal parenchyma. This kidney had never developed and therefore this process represents hypoplasia. How does one differentiate between atrophy and hypoplasia? | File:IPLab2Atrophy9.jpg|The two kidneys in this slide are from the same patient. One kidney (1) is relatively normal, although increased in size due to compensatory hypertrophy. The other kidney (2) is very small with only rudimentary nodules of renal parenchyma. This kidney had never developed and therefore this process represents hypoplasia. How does one differentiate between atrophy and hypoplasia? | ||
File:IPLab2Atrophy10.jpg|This gross photograph shows a normal brain (left) and a brain from a geriatric patient (right). Note the decreased size, the narrowed gyri, and the widened sulci of the brain from this octogenarian. What is the cause of atrophy in this case? | File:IPLab2Atrophy10.jpg|This gross photograph shows a normal brain (left) and a brain from a geriatric patient (right). Note the decreased size, the narrowed gyri, and the widened sulci of the brain from this octogenarian. What is the cause of atrophy in this case? | ||
| + | </gallery> | ||
| − | </ | + | == Study Questions == |
| + | * <spoiler text="What is PSA and how useful is it as a marker of prostatic cancer?">Prostatic Specific Antigen. PSA can be a useful marker for prostatic cancer; however, PSA levels may be elevated for a number of reasons other than cancer.</spoiler> | ||
| + | * <spoiler text="What is the cause of testicular atrophy in this case?">The cause was HORMONAL. | ||
| + | |||
| + | Prostatic growth is dependent upon testicular androgens. Estrogen therapy leads to inhibition of pituitary gonadotropin and/or ACTH production which causes androgen deprivation. Newer drugs use specific testosterone receptor blocking mechanisms to regress prostate hyperplasia and prostate cancer.</spoiler> | ||
| + | * <spoiler text=" "> </spoiler> | ||
| + | * <spoiler text=" "> </spoiler> | ||
{{IPLab 2}} | {{IPLab 2}} | ||
[[Category: IPLab:Lab 2]] | [[Category: IPLab:Lab 2]] | ||
Revision as of 15:01, 21 August 2013
Clinical Summary[edit]
This 74-year-old man was found to have carcinoma of the prostate six years prior to his death. The serum prostate-specific antigen (PSA) level was 9.7 ng/ml. His plasma acid phosphatase level on repeated tests ranged from 2 to 4 IU/L. X-rays revealed metastatic lesions in the patient's pelvis and vertebral column. He refused to have an orchiectomy and was placed on estrogen therapy (diethylstilbestrol).
The patient's terminal admission was for renal failure. The tumor had grown into the floor of the urinary bladder causing obstruction of the ureters at their entrance to the bladder. The patient developed acute hydronephrosis which was drained by nephrostomies. Eventually, infection developed in the kidneys resulting in Gram-negative sepsis and death.
Images[edit]
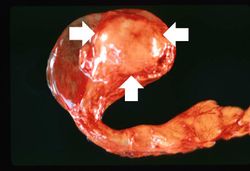
This is a gross photograph of an atrophied testis (arrows).
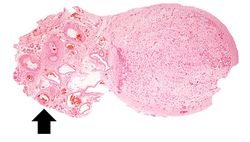
This is a low-power photomicrograph of an atrophic testis. Attached to the testis are several vessels (arrow) which are part of the epididymis and the vas deferens.
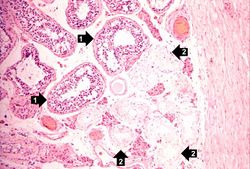
This is a higher-power photomicrograph of an atrophic testis. In this section there are seminiferous tubules with viable cells (1) although there are no visible spermatocytes. Other seminiferous tubules are completely acellular and have a pale pink hyaline appearance (2).
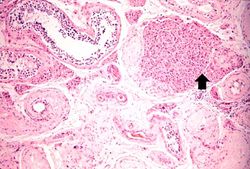
This is a higher-power photomicrograph indicating loss of testicular parenchymal tissue. There are very few recognizable spermatic cells in this tissue. The cluster of cells in the upper right is a focus of interstitial or Leydig cells (arrow). These cells are not affected by the hormone-induced atrophy process.
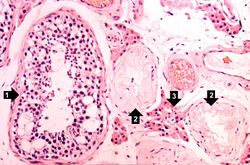
A seminiferous tubule is shown on the left containing remnants of spermatocytes (1). There are no mature sperm present. On the right-hand portion of the slide are remnants of other spermatic tubules which have completely atrophied and lost all of their spermatogenic cells (2). Note the eosinophilic Leydig cells present between the atrophic tubules (3).
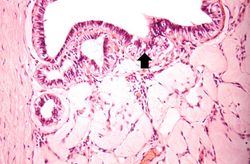
In this slide, the atrophy of the tubules is extending to include the Rete testes (arrow) as well.
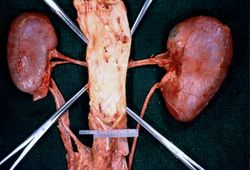
In this gross photograph of kidneys and the abdominal aorta, there is narrowing of the left renal artery at its ostium from the aorta. This atherosclerotic narrowing of the renal artery causes reduced blood pressure in the kidney whose artery is affected. The result is a characteristic Goldblatt’s hypertension syndrome. Note that the kidney with the narrowed renal artery is atrophied compared to the kidney with the normal vessel on the right. What is the cause of the atrophy in this kidney?

These kidneys were removed from a patient who had blockage of one ureter leading to increased pressure in the renal pelvis. The increased pressure produced hydronephrosis (arrow) in one kidney. What is the cause of atrophy in this case?

The two kidneys in this slide are from the same patient. One kidney (1) is relatively normal, although increased in size due to compensatory hypertrophy. The other kidney (2) is very small with only rudimentary nodules of renal parenchyma. This kidney had never developed and therefore this process represents hypoplasia. How does one differentiate between atrophy and hypoplasia?

This gross photograph shows a normal brain (left) and a brain from a geriatric patient (right). Note the decreased size, the narrowed gyri, and the widened sulci of the brain from this octogenarian. What is the cause of atrophy in this case?










Study Questions[edit]
| |||||
Prostate-specific antigen (PSA) is a product of prostate epithelium which is normally emitted in the semen. Normal men have very low levels of PSA circulating in their blood. PSA levels are slightly raised in men who have prostatic hyperplasia but are greatly elevated in men who have prostate cancer (the level increases proportionately to the severity of the cancer). PSA is a useful marker for both localized and metastatic prostate cancer.
A PSA level above 4 ng/ml should lead to suspicion of prostate cancer.
Plasma acid phosphatase is a useful marker for metastatic prostate cancer but not for localized prostate cancer.
A normal level should be less than 0.8 IU/L.
An orchiectomy is the surgical removal of a testicle. The growth of a prostatic carcinoma is androgen-dependent. Removal of the testes (hence removal of androgens) can lead to tumor regression--although usually temporary.
Since prostatatic carcinomas are androgen-dependent, estrogen therapy helps to reduce output of testosterone thereby slowing tumor progression.
Renal failure is the severe reduction of renal function and often leads to reduced urinary output.
Hydronephrosis is dilation of the renal pelvis and atrophy of the cortex due to increase pressure from retained urine.
A nephrostomy is the creation of a permanent opening directly into the renal pelvis to allow the drainage of urine.
Gram-negative sepsis is a systemic inflammatory response caused by the presence of Gram-negative bacteria and their endotoxins in the blood. The microbes usually enter the bloodstream from an area of localized infection. Gram-negative sepsis is the leading cause of septic shock--hence, also known as "endotoxic shock." Septic shock is a syndrome of inflammatory responses which can lead to severe hypotension, multiple organ system failure, and death.
Atherosclerosis is the deposition of lipid into the intima of arteries, resulting in narrowing of the vessel lumen.