Difference between revisions of "IPLab:Lab 3:Healed Myocardial Infarction"
Seung Park (talk | contribs) |
(→Clinical Summary) |
||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| − | This | + | This 57-year-old white female with a 22 year history of insulin-dependent diabetes was admitted to the hospital 10 hours prior to death complaining of shortness of breath. Three months before, she had begun to experience progressive weakness and for the previous 3 weeks she noticed increasing dyspnea on exertion and worsening of a chronic cough. Despite appropriate care she developed an intractable arrhythmia and could not be resuscitated. |
| + | |||
| + | Autopsy showed a 340-gram heart with extensive transmural reddish discoloration of the anterolateral portion of the myocardium of the left ventricle. There was severe atherosclerotic narrowing of all coronary arteries and an acute thrombus in the left anterior descending. The lungs showed pulmonary edema and early bronchopneumonia. | ||
== Autopsy Findings == | == Autopsy Findings == | ||
Revision as of 01:16, 24 June 2020
Contents
Clinical Summary[edit]
This 57-year-old white female with a 22 year history of insulin-dependent diabetes was admitted to the hospital 10 hours prior to death complaining of shortness of breath. Three months before, she had begun to experience progressive weakness and for the previous 3 weeks she noticed increasing dyspnea on exertion and worsening of a chronic cough. Despite appropriate care she developed an intractable arrhythmia and could not be resuscitated.
Autopsy showed a 340-gram heart with extensive transmural reddish discoloration of the anterolateral portion of the myocardium of the left ventricle. There was severe atherosclerotic narrowing of all coronary arteries and an acute thrombus in the left anterior descending. The lungs showed pulmonary edema and early bronchopneumonia.
Autopsy Findings[edit]
Autopsy showed a 340-gram heart with extensive transmural reddish discoloration of the anterolateral portion of the myocardium of the left ventricle. There was severe atherosclerotic narrowing of all coronary arteries especially the left anterior descending. The lungs showed pulmonary edema and early bronchopneumonia.
Images[edit]
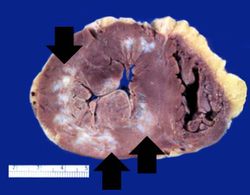
This is a gross photograph of a heart with areas of old healed myocardial infarction (scars) outlined by arrows.
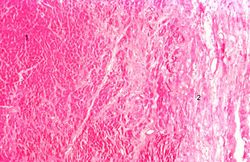
This is a low-power photomicrograph of a healed myocardial infarction with a fibrous scar. Remaining normal tissue is on the left (1) and the fibrous connective tissue scar is on the right (2).
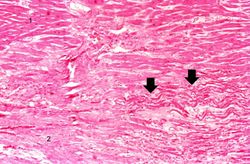
This is a higher-power photomicrograph of a healed myocardial infarction with a fibrous scar. Remaining normal tissue is at the top (1) and the fibrous connective tissue scar is at the bottom (2). Note the presence of occasional hypereosinophilic myocytes indicating recent acute ischemic injury to this region of old scar tissue (arrows).
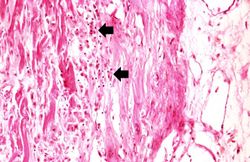
This is another high-power photomicrograph of a healed myocardial infarction. Note the remaining normal myocytes (1), the fibrous connective tissue (2), and occasional hypereosinophilic myocytes indicating recent acute ischemic injury (arrow).
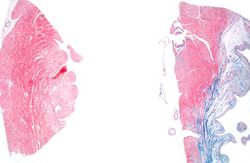
This is a low-power photomicrograph of two sections of myocardial tissue stained with a trichrome stain to demonstrate fibrous connective tissue (blue). The section on the left is from a heart with a recent myocardial infarction. Notice the absence of fibrous connective tissue. The section on the right is from a heart with an old healed infarct and it contains extensive fibrous connective tissue scars.
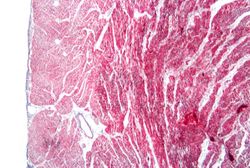
This is a photomicrograph of a trichrome-stained section from a heart with an acute myocardial infarction. Note that there is little fibrous connective tissue. It is too early for scar formation to have taken place in this acute lesion.

This is a photomicrograph of a trichrome-stained section of heart containing an old healed myocardial infarction. The scar is composed of mature fibrous connective tissue (arrows).

This is a higher-power photomicrograph of a trichrome-stained section of heart containing an old healed MI. The scar tissue (mature fibrous connective tissue) is stained blue.








Virtual Microscopy[edit]
Early (Inflammatory Response)[edit]
Late (Replacement Fibrosis)[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
Journal Articles[edit]
- Yuan S, Liu Y, Zhu L. Vascular complications of diabetes mellitus. Clin Exp Pharmacol Physiol 1999 Dec;26(12):977-8.
Images[edit]
Related IPLab Cases[edit]
- Lab 1: Heart: Myocardial Infarction (Coagulative Necrosis)
- Lab 3: Heart: Acute Myocardial Infarction
- Lab 4: Heart: Mural Thrombus
- Lab 4: Coronary Artery: Thrombosis
- Lab 4: Lung: Pulmonary Congestion and Edema
Shortness of breath is a common clinical manifestation of heart failure.
A normal heart weighs 300 grams (range: 270 to 360 grams).
Atherosclerosis is the deposition of lipid into the intima of arteries, resulting in narrowing of the vessel lumen.
A thrombus is a solid mass resulting from the aggregation of blood constituents within the vascular system.
Pulmonary edema refers to the accumulation of fluid in the pulmonary alveolar and tissue spaces as a result of changes in capillary permeability and/or increases in capillary hydrostatic pressure.
Myocardial infarction is necrosis of myocardial tissue which occurs as a result of a deprivation of blood supply, and thus oxygen, to the heart tissue. Blockage of blood supply to the myocardium is caused by occlusion of a coronary artery.
An occlusion is a blockage.
An infiltrate is an accumulation of cells in the lung parenchyma--this is a sign of pneumonia.
A normal partial thromboplastin time is 28 to 37 seconds.