Difference between revisions of "IPLab:Lab 5:Neurofibromatosis"
Seung Park (talk | contribs) |
Seung Park (talk | contribs) |
||
| Line 15: | Line 15: | ||
File:IPLab5Neurofibromatosis7.jpg|This higher-power photomicrograph of the neurofibroma shows more clearly the elongated cells (primarily Schwann cells) that make up this tumor. | File:IPLab5Neurofibromatosis7.jpg|This higher-power photomicrograph of the neurofibroma shows more clearly the elongated cells (primarily Schwann cells) that make up this tumor. | ||
File:IPLab5Neurofibromatosis8.jpg|This is a high-power photomicrograph of the cells in the neurofibroma. | File:IPLab5Neurofibromatosis8.jpg|This is a high-power photomicrograph of the cells in the neurofibroma. | ||
| + | </gallery> | ||
| − | </ | + | == Study Questions == |
| + | * <spoiler text="What type of neurofibromatosis is this?">This is type 1 neurofibromatosis (von Recklinghausen disease). There is no eighth nerve involvement as is seen in Type 2 or acoustic neurofibromatosis.</spoiler> | ||
| + | * <spoiler text="What is the significance of no positive family history in this patient with type 1 neurofibromatosis?">Neurofibromatosis type 1 is an autosomal dominant disorders with a frequency of almost 1 in 3000. The gene that causes neurofibromatosis type 1 has been mapped to chromosome 17q11. This gene encodes a protein called neurofibromin, which down-regulates the function of the p21 ras oncoprotein. Approximately 50% of affected patients have a definite family history consistent with autosomal dominant transmission, however, the remaining cases appear to be caused by new mutations. This case may represent a new mutation.</spoiler> | ||
| + | * <spoiler text="What are the classic clinical features of neurofibromatosis type 1?">Although protean in its clinical expression, patients with neurofibromatosis usually have multiple neural tumors all over the body, numerous pigmented skin lesions (”café au lait“ spots), and pigmented iris hamartomas (also called Lisch nodules). Other common clinical manifestations include skeletal lesions (scoliosis, bone cysts, thinning of the cortex of long bones) and mild intellectual impairment.</spoiler> | ||
| + | * <spoiler text="What is the etiology of the coagulopathy seen in this patient?">Liver failure.</spoiler> | ||
{{IPLab 5}} | {{IPLab 5}} | ||
[[Category: IPLab:Lab 5]] | [[Category: IPLab:Lab 5]] | ||
Revision as of 15:05, 21 August 2013
Clinical Summary[edit]
This 45-year-old divorced white male came to the emergency room with severe hepatic cirrhosis and aspiration pneumonia. Shortly after admission he developed cardiac arrhythmias and died. Significant past history included alcohol abuse, cirrhosis, and neurofibromatosis. He had no family history of neurofibromatosis, but his condition was diagnosed at age 17 when he developed neurofibromas along the lateral chest wall. There was no history of continued follow-up after this initial diagnosis.
Autopsy Findings[edit]
The patient was covered with variably sized subcutaneous nodules ranging from 0.5 to 2.5 cm in diameter. Other significant findings included micronodular hepatic cirrhosis (liver weight: 1760 grams), ascites (500 ml), and splenomegaly (weight: 260 grams).
Images[edit]

This photograph, taken at autopsy, demonstrates the distribution of neurofibromas on the skin of this patient.

This is another view taken at autopsy demonstrating the neurofibromas. Some lesions can be seen as subcutaneous swellings (arrow) and others form pedunculated masses. Most are hyperpigmented.

This is a closer view of neurofibromas on the skin.
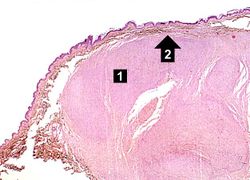
This is a low-power photomicrograph of a subcutaneous neurofibroma (1). Note the increased pigmentation in the skin (2).
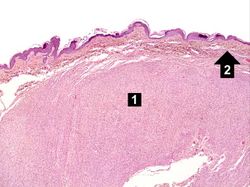
This is a higher-power photomicrograph of the neurofibroma (1) with the overlying skin (2).
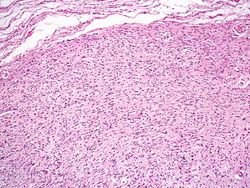
This is a higher-power photomicrograph of the neurofibroma demonstrating the loose pattern of elongated cells making up the tumor mass.
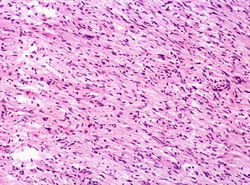
This higher-power photomicrograph of the neurofibroma shows more clearly the elongated cells (primarily Schwann cells) that make up this tumor.
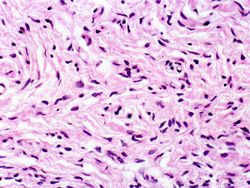
This is a high-power photomicrograph of the cells in the neurofibroma.








Study Questions[edit]
| |||||
Cirrhosis is a liver disease characterized by necrosis, fibrosis, loss of normal liver architecture, and hyperplastic nodules.
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.
Arrhythmias are abnormal heart rhythms.
A normal liver weighs 1650 grams (range: 1500 to 1800 grams).
Ascities is the accumulation of fluid with in the abdominal cavity. There should be less than 30 ml of fluid in the peritoneal cavity.
260 grams)
Splenomegaly means enlargement of the spleen. The normal spleen weighs 155 grams.