IPLab:Lab 11:Malaria
Contents
Clinical Summary
This 46-year-old forestry consultant presented with a seven-day history of mild abdominal cramping, diarrhea, mild myalgias, gradually worsening headache, and subjective fever. The patient had recently returned from spending 5 months in the Thailand rainforests as a consultant to lumber companies. Stool cultures and repeated stool examinations for ova and parasites were negative. A presumptive diagnosis of viral gastroenteritis was made. Three days later the patient returned with a fever of 103° and bloody diarrhea. On examination the patient appeared acutely ill and had orthostatic hypotension. Exam was otherwise unremarkable. The patient was admitted and intravenous rehydration and broad-spectrum IV antibiotics were begun. Over the next eight hours the patient became progressively lethargic and finally became unresponsive to speech. His temperature rose to 106°. Careful examination of a peripheral blood smear revealed P. falciparum with a parasitemia of 5%. Intravenous antimalarial drugs were administered and over the next three days the patient's clinical condition gradually improved. Repeat peripheral smears at 3, 7, 14, and 28 days were negative for malaria.
Images
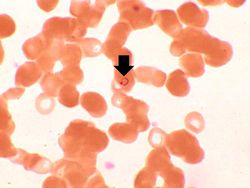
This is a high power photomicrograph of a thin smear of blood from this patient. Note that one of the RBCs has a ring stage trophozoite (arrow).
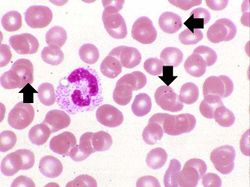
This is another high power photomicrograph of a thin smear of blood from this patient. There is a single eosinophil in this smear along with several RBCs containing ring stage trophozoites (arrows).
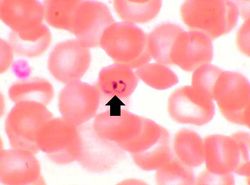
This is yet another high power photomicrograph of a thin smear of blood from this patient. There is one RBC that contains two ring stage trophozoites (arrow). This is characteristic of, but not diagnostic for, P. falciparum.
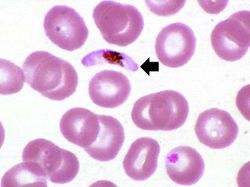
In this high power photomicrograph of a thin smear of blood from this patient there is one P. falciparum gametocyte (arrow). These gametocytes have a characteristic "banana" shape.
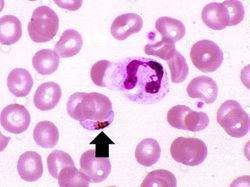
There is another example of a P. falciparum gametocyte (arrow) in this thin smear. There is a neutrophil in this field as well.
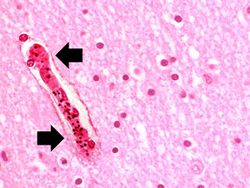
This high photomicrograph was taken from another patient who died of malignant cerebral malaria caused by P. falciparum. In this photomicrograph, a small artery (arrow) can be seen that is full of parasitized RBCs. These RBCs tend to clog small blood vessels and lead to cerebral ischemia/hypoxia.
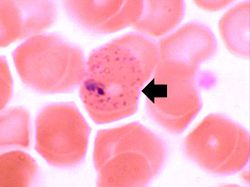
In this peripheral smear from a different patient who was infected with P. vivax, the cytoplasm of the infected RBC has a stippled appearance (Schüffner's dots) (arrow). The RBC is also slightly enlarged.







Virtual Microscopy
Study Questions
Additional Resources
Reference
- eMedicine Medical Library: Malaria
- eMedicine Medical Library: Emergent Management of Malaria
- Merck Manual: Malaria
- Centers for Disease Control and Prevention: Parasites
Journal Articles
- Mishra SK, Mohanty S, Mohanty A, Das BS. Management of severe and complicated malaria. J Postgrad Med 2006 Oct-Dec;52(4):281-7.
Images
| |||||