Difference between revisions of "IPLab:Lab 4:Thrombosis"
Seung Park (talk | contribs) (→Images) |
(→Images) |
||
| (5 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| + | This 83-year-old male developed chest pain. He had been awakened the previous night with dull chest pain which was retrosternal and radiated through to his back. The pain was associated with sweating, nausea, and vomiting and could not be relieved by antacids. He refused to go to the doctor but the next morning he developed severe epigastric pain and had several episodes of tachycardia (150-160 beats per minute) and later cardiac standstill. He had a history of hypertension and diabetes. | ||
| − | + | At autopsy the heart weighed 500 grams. There was massive acute myocardial infarction (about 2 days old) involving the posterior left ventricle, interventricular septum, and right ventricle from apex to base. The infarct was transmural, and there was a small rupture in the soft infarcted area at the apex. There were 1200 mL of blood within the right pleural cavity, probably secondary to this rupture. The coronary arteries showed moderate to severe atherosclerosis throughout the coronary tree. | |
| − | |||
| − | |||
| − | |||
| − | |||
== Images == | == Images == | ||
<gallery heights="250px" widths="250px"> | <gallery heights="250px" widths="250px"> | ||
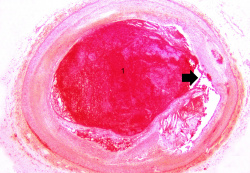
File:IPLab4Thrombosis1.jpg|This is a gross photograph of thrombosed coronary artery (arrows). | File:IPLab4Thrombosis1.jpg|This is a gross photograph of thrombosed coronary artery (arrows). | ||
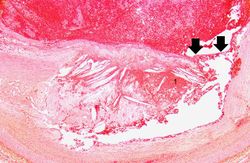
| − | File: | + | File:IPLab4Thrombosis2x.jpg|This is a low-power photomicrograph of thrombosed coronary artery. The thrombus (1) completely occludes the vessel. Note the layering of the thrombus. The fibrous cap is ruptured (arrow) and there is hemorrhage into the atherosclerotic plaque. Note the cholesterol crystals in the plaque. |
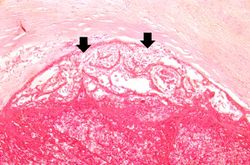
File:IPLab4Thrombosis3.jpg|This is a higher-power photomicrograph of the ruptured fibrous cap (arrows) with hemorrhage (1) into the atherosclerotic plaque. | File:IPLab4Thrombosis3.jpg|This is a higher-power photomicrograph of the ruptured fibrous cap (arrows) with hemorrhage (1) into the atherosclerotic plaque. | ||
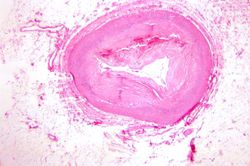
File:IPLab4Thrombosis4.jpg|This is another high-power photomicrograph of the ruptured fibrous cap (arrows) with hemorrhage (1) into the atherosclerotic plaque. Note the presence of cholesterol crystals. | File:IPLab4Thrombosis4.jpg|This is another high-power photomicrograph of the ruptured fibrous cap (arrows) with hemorrhage (1) into the atherosclerotic plaque. Note the presence of cholesterol crystals. | ||
| Line 20: | Line 17: | ||
File:IPLab4Thrombosis10.jpg|This is a high-power photomicrograph of the luminal surface of a re-canalized vessel. Note that the vessel lumen is lined by endothelial cells (arrows). | File:IPLab4Thrombosis10.jpg|This is a high-power photomicrograph of the luminal surface of a re-canalized vessel. Note that the vessel lumen is lined by endothelial cells (arrows). | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Virtual Microscopy == | ||
| + | <peir-vm>IPLab4Thrombosis</peir-vm> | ||
== Study Questions == | == Study Questions == | ||
Latest revision as of 19:23, 8 July 2020
Contents
Clinical Summary[edit]
This 83-year-old male developed chest pain. He had been awakened the previous night with dull chest pain which was retrosternal and radiated through to his back. The pain was associated with sweating, nausea, and vomiting and could not be relieved by antacids. He refused to go to the doctor but the next morning he developed severe epigastric pain and had several episodes of tachycardia (150-160 beats per minute) and later cardiac standstill. He had a history of hypertension and diabetes.
At autopsy the heart weighed 500 grams. There was massive acute myocardial infarction (about 2 days old) involving the posterior left ventricle, interventricular septum, and right ventricle from apex to base. The infarct was transmural, and there was a small rupture in the soft infarcted area at the apex. There were 1200 mL of blood within the right pleural cavity, probably secondary to this rupture. The coronary arteries showed moderate to severe atherosclerosis throughout the coronary tree.
Images[edit]

This is a gross photograph of thrombosed coronary artery (arrows).
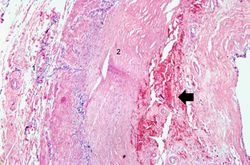
This is a low-power photomicrograph of thrombosed coronary artery. The thrombus (1) completely occludes the vessel. Note the layering of the thrombus. The fibrous cap is ruptured (arrow) and there is hemorrhage into the atherosclerotic plaque. Note the cholesterol crystals in the plaque.
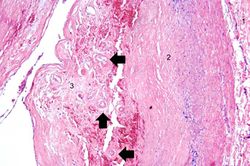
This is a higher-power photomicrograph of the ruptured fibrous cap (arrows) with hemorrhage (1) into the atherosclerotic plaque.

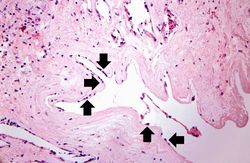
This is another high-power photomicrograph of the ruptured fibrous cap (arrows) with hemorrhage (1) into the atherosclerotic plaque. Note the presence of cholesterol crystals.

This is a high-power photomicrograph of thrombus attached to the wall of the vessel. There is early organization of the thrombus (arrow).
This is a higher-power photomicrograph of thrombus attached to the wall of the vessel. Note the early organization with in-growth of fibroblasts and small blood vessels from the wall of the artery (arrows).
In this low-power photomicrograph of another coronary artery from this patient, a mural thrombus has undergone re-organization. The mural thrombus has been invaded by the in-growth of fibroblasts and small blood vessels from the wall of the artery. The thrombotic material has been phagocytosed and removed by macrophages and is replaced by fibrous connective tissue and blood vessels. This re-organized thrombus still compromises the lumen of this vessel.
This is a higher-power photomicrograph of the vessel wall. The adventitia (1) and the media (2) contain inflammatory cells. The recanalized portion of the vessel is composed of fibrous connective tissue and contains numerous small blood vessels. There is a small area of hemorrhage (arrow) in the central portion of this image.
This is a higher-power photomicrograph of another region of the vessel wall. The adventitia (1) and the media (2) contain inflammatory cells. The recanalized portion of the vessel (3) is composed of fibrous connective tissue and contains numerous small blood vessels (arrows).
This is a high-power photomicrograph of the luminal surface of a re-canalized vessel. Note that the vessel lumen is lined by endothelial cells (arrows).










Virtual Microscopy[edit]
Study Questions[edit]
- What is the source for the fibroblasts and endothelial cells that are present in organizing thrombi?
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Noncoronary Atherosclerosis
- eMedicine Medical Library: Myocardial Infarction
- Merck Manual: Thrombotic Disorders
- Merck Manual: Acute Coronary Syndromes (ACS)
Journal Articles[edit]
- Jaeger BR. Evidence for maximal treatment of atherosclerosis: drastic reduction of cholesterol and fibrinogen restores vascular homeostasis. Ther Apher 2001 Jun;5(3):207-11.
Images[edit]
Related IPLab Cases[edit]
- Lab 1: Heart: Myocardial Infarction (Coagulative Necrosis)
- Lab 3: Heart: Acute Myocardial Infarction
- Lab 3: Heart: Healed Myocardial Infarction
- Lab 4: Heart: Mural Thrombus
- Lab 4: Lung: Pulmonary Congestion and Edema
| |||||
Myocardial infarction is necrosis of myocardial tissue which occurs as a result of a deprivation of blood supply, and thus oxygen, to the heart tissue. Blockage of blood supply to the myocardium is caused by occlusion of a coronary artery.
A thrombus is a solid mass resulting from the aggregation of blood constituents within the vascular system.
Mural thrombosis is the formation of multiple thrombi along an injured endocardial wall.
Recanalization is the process of the forming of channels through an organized thrombus so that blood flow is restored.
An occlusion is a blockage.