Difference between revisions of "IPLab:Lab 3:Brain Infarction"
(→Images) |
(→Images) |
||
| Line 9: | Line 9: | ||
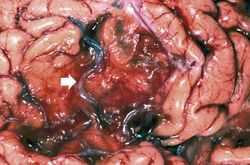
File:IPLab3BrainInfarction2.jpg|This is a gross photograph of a cross-section of brain demonstrating the areas of infarction (arrows). | File:IPLab3BrainInfarction2.jpg|This is a gross photograph of a cross-section of brain demonstrating the areas of infarction (arrows). | ||
File:IPLab3BrainInfarction3b.JPG|This is a low-power photomicrograph of this brain with several areas of infarcted tissue. Note the pale areas which correspond to areas with loss of brain parenchyma (arrows). | File:IPLab3BrainInfarction3b.JPG|This is a low-power photomicrograph of this brain with several areas of infarcted tissue. Note the pale areas which correspond to areas with loss of brain parenchyma (arrows). | ||
| − | File:IPLab3BrainInfarction4b.JPG|This | + | File:IPLab3BrainInfarction4b.JPG|This photomicrograph shows the area of healed/healing infarction (I) and more normal brain parenchyma (B). |
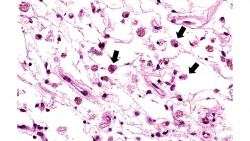
File:IPLab3BrainInfarction5b.JPG|This is a higher-power photomicrograph of the previous image showing that the inflammatory cells (arrows) are primarily macrophages and microglia which have phagocytosed the dead brain tissue. | File:IPLab3BrainInfarction5b.JPG|This is a higher-power photomicrograph of the previous image showing that the inflammatory cells (arrows) are primarily macrophages and microglia which have phagocytosed the dead brain tissue. | ||
File:IPLab3BrainInfarction6b.JPG|This is a photomicrograph of brain tissue adjacent to the area of infarction. There are numerous activated gemistocytic astrocytes (arrows). | File:IPLab3BrainInfarction6b.JPG|This is a photomicrograph of brain tissue adjacent to the area of infarction. There are numerous activated gemistocytic astrocytes (arrows). | ||
Revision as of 22:34, 23 June 2020
Contents
Clinical Summary[edit]
Eight years prior to his demise, this 48-year-old black male had a dissecting aortic aneurysm. The first portion of the aortic arch was dilated and he had associated aortic valve insufficiency. The defect was repaired and a mechanical prosthetic aortic valve was implanted. One year prior to his terminal admission, the patient experienced a catastrophic cerebrovascular accident (CVA) with left hemiparesis and obtundation. The patient experienced severe neurologic sequelae from this CVA and was eventually transferred to a nursing home where he was bedbound and required an indwelling urinary catheter. Four months later the patient developed a urinary tract infection and was transferred to the hospital. The patient's condition deteriorated with a urinary tract infection and pneumonia and he died of sepsis.
Autopsy showed the expected findings in the aorta and in a 760-gram heart. The mechanical valve showed some old thrombotic material adherent to the valve which was probably the source of the emboli which caused the patient's CVA. The patient's 1250-gram brain showed extensive old infarctions in at least three different areas, with the largest (12.5 x 5.5 cm) in the distribution of the right middle cerebral artery.
Images[edit]

This is a gross photograph of the brain which contains two areas of infarction (arrows).

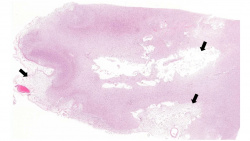
This is a gross photograph of a cross-section of brain demonstrating the areas of infarction (arrows).
This is a low-power photomicrograph of this brain with several areas of infarcted tissue. Note the pale areas which correspond to areas with loss of brain parenchyma (arrows).
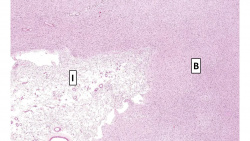
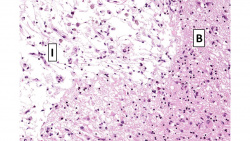
This photomicrograph shows the area of healed/healing infarction (I) and more normal brain parenchyma (B).
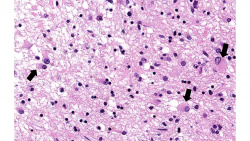
This is a higher-power photomicrograph of the previous image showing that the inflammatory cells (arrows) are primarily macrophages and microglia which have phagocytosed the dead brain tissue.
This is a photomicrograph of brain tissue adjacent to the area of infarction. There are numerous activated gemistocytic astrocytes (arrows).
This is a photomicrograph of the edge of the infarct. The macrophages that are full of brain tissue (“gitter cells”) are at the top of the image (arrows) and the brain parenchyma containing gemistocytic astrocytes is at the bottom.

This is a gross photograph of a brain from another patient with an old healed infarct. Note the meninges overlying the infarcted region (arrow).
This is a closer view of the brain demonstrating an old healed infarct with the meninges containing blood vessels (arrow) overlying the infarcted region.









Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Ischemic Stroke
- eMedicine Medical Library: Acute Aortic Dissection
- eMedicine Medical Library: Prosthetic Heart Valves
- Merck Manual: Overview of Stroke (CVA)
- Merck Manual: Thrombotic Disorders
- Merck Manual: Aortic Dissection
Journal Articles[edit]
- Love S, Barber R, Wilcock GK. Neuronal death in brain infarcts in man. Neuropathol Appl Neurobiol 2000 Feb;26(1):55-66.
Images[edit]
Related IPLab Cases[edit]
A dissecting aortic aneurysm occurs when an intimal tear allows blood--under very high pressure--to enter the media and thus to separate the intima from the adventitia. The separation occurs longitudinally and amounts to the formation of a blood-filled canal parallel to the aortic lumen which may run the entire length of the aorta. The word aneurysm usually refers to an abnormal dilatation of a localized segment of artery. Since marked dilatation of the aorta is not a prominent feature of a dissecting lesion, aortic dissection is now the preferred term.
Aortic insufficiency refers to the inability of the aortic valve to close properly, thus allowing regurgitation of blood into the left ventricle during diastole -- i.e., volume overload. Disease of the aortic valve leaflets is a common cause of insufficiency.
A cerebrovascular accident (CVA) is known as a stroke in layman's terms. The most common cause of CVAs, by far, is a brain infarction resulting from reduced blood flow secondary to a thrombotic embolus (blood clot).
Slight paralysis or weakness affecting one side of the body.
Obtunded patients will have mental blunting with mild to moderate reduction in alertness and a diminished sensation of pain.
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.
A normal heart weighs 300 grams (range: 270 to 360 grams).
Plural of embolus. An embolus is something that blocks the blood flow in a blood vessel. It may be a gas bubble, a blood clot, a fat globule, a mass of bacteria, or other foreign body. It usually forms somewhere else and travels through the circulatory system until it gets stuck.
A normal brain weighs 1400 grams (range: 1100 to 1700 grams).
Gemistocytic astrocytes (gemistocytes) comprise a form of activated astrocyte in which the cell body becomes round and swollen, the nucleus assumes an eccentric position, and the cytoplasm changes to an easily visible bright pink color.
An occlusion is a blockage.
A thrombus is a solid mass resulting from the aggregation of blood constituents within the vascular system.
A normal partial thromboplastin time is 28 to 37 seconds.