Difference between revisions of "IPLab:Lab 1:Fat Necrosis"
Seung Park (talk | contribs) (Created page with "== Clinical Summary == This was a 37-year-old female with chronic renal failure that necessitated a renal transplant. Following transplantation, the patient developed a herpes...") |
(→Images) |
||
| (14 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| − | This was a 37-year-old female with chronic renal failure | + | This was a 37-year-old female with chronic renal failure who underwent a cadaveric renal transplant. Following transplantation she developed oral candidiasis, pneumonia, pyuria, and gastrointestinal bleeding. Subsequently, the patient became septic and died. |
| + | |||
| + | Major findings at autopsy included extensive hemorrhagic bronchopneumonia and multiple ulcers affecting the stomach and esophagus. There was also evidence of disseminated intravascular coagulation (DIC) with multiple hemorrhages present. Firm, whitish foci of necrotic tissue were found in the fat around the pancreas. | ||
| − | == | + | == Images == |
| − | + | <gallery heights="250px" widths="250px"> | |
| + | File:IPLab1FatNecrosis1.jpg|This gross photograph shows the intestines and omentum at autopsy. Note the small (5-15 mm in diameter) white nodules on the surface of the omental and mesenteric fat tissue (arrows). | ||
| + | File:IPLab1FatNecrosis2.jpg|This gross photograph of the pancreas from this case shows white nodules (arrows) in the pancreas and the adjacent mesenteric fat tissue. | ||
| + | File:IPLab1FatNecrosis3.jpg|This low-power photomicrograph of the pancreas from this case shows the fat tissue (1) surrounding the pancreas. Note the rim of inflammatory cells (arrows) and the blue areas that represent calcified fat adjacent to the pancreas (2). | ||
| + | File:IPLab1FatNecrosis5.jpg|This medium-power photomicrograph shows the blue discoloration of the fat tissue in the interlobular spaces (1) of the pancreas. This blue to purple staining represents calcium deposits that occur after enzymatic necrosis of the fat cells releases free fatty acids. | ||
| + | File:IPLab1FatNecrosis6.jpg|A higher-power photomicrograph of the previous slide contains a small area of fat necrosis (1) in the upper right portion of the image. The fat necrosis is within the fat tissue that is normally found adjacent to the pancreas. The appearance of the pancreatic tissue in this area is somewhat disrupted due to autolysis (the pancreas autolyzes very rapidly after death) but there is some premortem necrosis as well. | ||
| + | File:IPLab1FatNecrosis10.jpg|This high-power photomicrograph demonstrates fat necrosis in the interlobular spaces of the pancreas. Note the granular blue-staining calcium deposits (arrows) within the fat cells. The clear areas represent artifact caused by the "washing-out" of fat from cells during tissue processing for histology. | ||
| + | </gallery> | ||
| + | |||
| + | == Virtual Microscopy == | ||
| + | === Pancreatic Fat Necrosis === | ||
| + | <peir-vm>IPLab1FatNecrosis</peir-vm> | ||
| − | == | + | === Normal Pancreas === |
| − | + | <peir-vm>UAB-Histology-00154</peir-vm> | |
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
== Study Questions == | == Study Questions == | ||
| Line 43: | Line 29: | ||
=== Reference === | === Reference === | ||
| − | * [http://emedicine.medscape.com/article/ | + | * [http://emedicine.medscape.com/article/775867-overview eMedicine Medical Library: Emergent Management of Pancreatitis] |
| − | * [http://www.merckmanuals.com/professional/ | + | * [http://www.merckmanuals.com/professional/gastrointestinal_disorders/pancreatitis/acute_pancreatitis.html Merck Manual: Acute Pancreatitis] |
=== Journal Articles === | === Journal Articles === | ||
| − | * | + | * Forsmark CE, Vege SS, Wilcox CM. [http://www.nejm.org/doi/full/10.1056/NEJMra1505202 Acute Pericarditis]. ''N Engl J Med" 2016; 375:1972-1981. November 17, 2016. |
| + | * LeWinter MM. [http://http://www.nejm.org/doi/full/10.1056/NEJMcp1404070 Acute Pericarditis]. ''NEJM'' 2014 Dec 18;371:2410-2416. | ||
=== Images === | === Images === | ||
| − | * [ | + | * [{{SERVER}}/library/index.php?/tags/333-pancreas PEIR Digital Library: Pancreas Images] |
| − | * [http://library.med.utah.edu/WebPath/ | + | * [http://library.med.utah.edu/WebPath/CINJHTML/CINJIDX.html WebPath: Cellular Injury Images] |
| − | |||
| − | |||
| − | |||
| − | |||
{{Template:IPLab 1}} | {{Template:IPLab 1}} | ||
| − | [[Category:IPLab]] | + | [[Category:IPLab:Lab 1]] |
Latest revision as of 18:34, 1 August 2019
Contents
Clinical Summary[edit]
This was a 37-year-old female with chronic renal failure who underwent a cadaveric renal transplant. Following transplantation she developed oral candidiasis, pneumonia, pyuria, and gastrointestinal bleeding. Subsequently, the patient became septic and died.
Major findings at autopsy included extensive hemorrhagic bronchopneumonia and multiple ulcers affecting the stomach and esophagus. There was also evidence of disseminated intravascular coagulation (DIC) with multiple hemorrhages present. Firm, whitish foci of necrotic tissue were found in the fat around the pancreas.
Images[edit]

This gross photograph shows the intestines and omentum at autopsy. Note the small (5-15 mm in diameter) white nodules on the surface of the omental and mesenteric fat tissue (arrows).

This gross photograph of the pancreas from this case shows white nodules (arrows) in the pancreas and the adjacent mesenteric fat tissue.
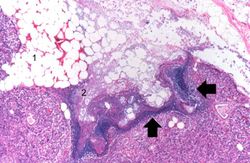
This low-power photomicrograph of the pancreas from this case shows the fat tissue (1) surrounding the pancreas. Note the rim of inflammatory cells (arrows) and the blue areas that represent calcified fat adjacent to the pancreas (2).
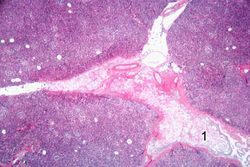
This medium-power photomicrograph shows the blue discoloration of the fat tissue in the interlobular spaces (1) of the pancreas. This blue to purple staining represents calcium deposits that occur after enzymatic necrosis of the fat cells releases free fatty acids.
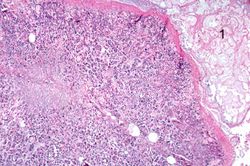
A higher-power photomicrograph of the previous slide contains a small area of fat necrosis (1) in the upper right portion of the image. The fat necrosis is within the fat tissue that is normally found adjacent to the pancreas. The appearance of the pancreatic tissue in this area is somewhat disrupted due to autolysis (the pancreas autolyzes very rapidly after death) but there is some premortem necrosis as well.
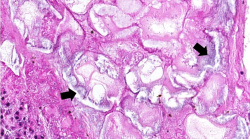
This high-power photomicrograph demonstrates fat necrosis in the interlobular spaces of the pancreas. Note the granular blue-staining calcium deposits (arrows) within the fat cells. The clear areas represent artifact caused by the "washing-out" of fat from cells during tissue processing for histology.






Virtual Microscopy[edit]
Pancreatic Fat Necrosis[edit]
Normal Pancreas[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
Journal Articles[edit]
- Forsmark CE, Vege SS, Wilcox CM. Acute Pericarditis. N Engl J Med" 2016; 375:1972-1981. November 17, 2016.
- LeWinter MM. Acute Pericarditis. NEJM 2014 Dec 18;371:2410-2416.
Images[edit]
| |||||
Renal failure is the severe reduction of renal function and often leads to reduced urinary output.
Candidiasis is an infection by the fungus Candida in the oral cavity.
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.
Pyuria is the presence of white blood cells (pus) in the urine.
Sepsis is the presence and persistence of pathogenic microorganisms and their toxins in the blood.
DIC is the development of small thrombi within the microcirculation throughout the body.