IPLab:Lab 9:Clostridial Myonecrosis
Contents
Clinical Summary[edit]
This 68-year-old white male with insulin-dependent diabetes was admitted one day before his death. The chief complaints were the occurrence of chills and fever since passing a kidney stone two days earlier. In the last day, the right leg had become swollen. The most striking physical findings were redness of the right posterior calf and crepitance in both legs. The patient's white blood cell count was found to be 34,000 cells/cmm and the packed red blood cell volume (PCV) was 18%. Within hours, the right calf became tense and the crepitance spread up to the nipple line. The patient vomited, aspirated the vomitus, and died 10 hours after admission.
Images[edit]

This gross photograph of the lower extremity was taken at autopsy. Notice the swelling and the area of the primary infection (arrow).

This gross photograph shows a close-up view of hemorrhagic blebs (arrows) on the skin. The blebs on the skin are accumulations of gas being discharged into the tissues from the Clostridium perfringens. This gas produces crepitance.
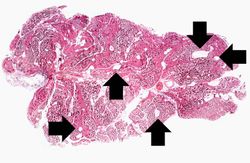
This is a low-power photomicrograph of muscle fascicles containing large gas bubbles (arrows). Note that there is no inflammatory reaction in this section.
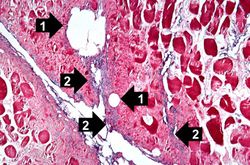
This is a high-power photomicrograph of skeletal muscle. The muscle cells are hypereosinophilic and most do not contain nuclei, indicating that these cells are dead or dying. The round clear spaces (1) in this tissue correspond to gas accumulations prior to death. In between the bundles of muscle cells, accumulations of small dark blue-staining bacterial organisms can be seen (2). Also note that there is no inflammatory response in this tissue.
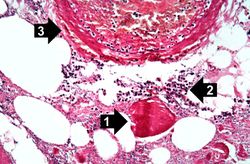
This high-power photomicrograph shows the gas accumulation present in the tissue, a necrotic muscle cell (1), and a mild inflammatory response (2). There is also a thrombosed blood vessel (3). The blue-staining rods (bacterial organisms) can barely be appreciated at this magnification.
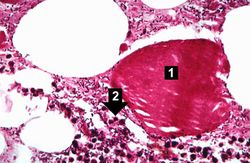
This higher-power photomicrograph of the previous image provides a clearer view of gas bubbles in the tissue, the necrotic hypereosinophilic muscle cell (1), and the mild inflammatory reaction (2). At this magnification, the bacteria located throughout this section can be better appreciated.
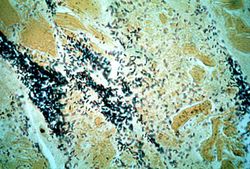
This is a high-power photomicrograph of a tissue section stained with a tissue Gram's stain (Brown & Brenn). The Gram-positive bacilli can be seen throughout this tissue section.







Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Clostridial Gas Gangrene
- eMedicine Medical Library: Gas Gangrene
- Merck Manual: Gas Gangrene
Images[edit]
Related IPLab Cases[edit]
| |||||
A normal hematocrit for a male is 39 to 49%.