Difference between revisions of "IPLab:Lab 3:Lobar Pneumonia"
(→Clinical Summary) |
(→Autopsy Findings) |
||
| Line 5: | Line 5: | ||
At autopsy the right lung weighed 800 grams. The most striking finding was a marked uniform consolidation of the entire middle lobe which was reddish-gray in color. There was also marked thickening of the pleura overlying the middle lobe. | At autopsy the right lung weighed 800 grams. The most striking finding was a marked uniform consolidation of the entire middle lobe which was reddish-gray in color. There was also marked thickening of the pleura overlying the middle lobe. | ||
| − | |||
| − | |||
| − | |||
== Images == | == Images == | ||
Latest revision as of 23:01, 19 June 2020
Contents
Clinical Summary[edit]
This 41-year-old black male was brought to the hospital in a comatose state. The patient, who had a history of heavy alcohol intake, was found comatose on the morning of the day of admission. No further history is available.
On admission, the pertinent findings included a temperature of 104°, a white cell count of 22,700 cells/mm³, nuchal rigidity, elevated spinal fluid pressure, and the presence of Gram-positive diplococci on a smear of spinal fluid (cultures of blood and spinal fluid were subsequently reported positive for Streptococcus pneumoniae). The patient expired 12 hours after admission in spite of intensive antibiotic therapy.
At autopsy the right lung weighed 800 grams. The most striking finding was a marked uniform consolidation of the entire middle lobe which was reddish-gray in color. There was also marked thickening of the pleura overlying the middle lobe.
Images[edit]

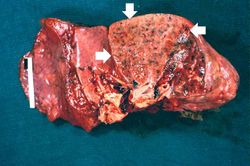
This is a gross photograph of the lungs from a patient (not the patient from this case) with acute lobar pneumonia. The lung lobe in the upper-right portion of the photograph is affected with pneumonia (arrows). It has a whitish discoloration and appears swollen compared to the more pink-staining normal lung lobe in the lower right and left-hand portions of this photograph.
This is a cut section of a lung from the preceding image. Note the whitish discoloration of the lung tissue in the upper lobe (arrows) compared to the normal collapsed and pink staining lung lobe in the left-hand portion of the photograph. The white discoloration in this tissue is due to infiltration of leukocytes (primarily neutrophils). Note that only one lobe of the lung is involved in this patient with lobar pneumonia.

This is a gross photograph of the right lung from the patient in this case. This lung shows complete consolidation with a marked infiltration of neutrophils throughout the tissue giving the lung a whitish discoloration. Note the extensive black pigment in this lung due to anthracosis. This is an advanced case of lobar pneumonia with extensive necrosis which obviously did not resolve, thus resulting in the death of the patient.
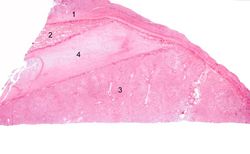
This low-power photomicrograph of the lung shows: (1) markedly thickened pleura, indicating an inflammatory process which has been present for several days; (2) a small wedge-shaped segment of normal lung which is somewhat compressed due to artifact; (3) a large wedge-shaped segment of lung tissue with lobar pneumonia, which appears very dense due to extensive cellular infiltrate; and (4) a greatly thickened pleural space between these two lung lobes. This interlobar space is markedly thickened due to deposition of fibrinous exudate.
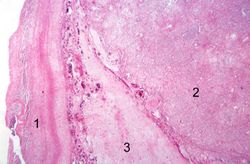
This is a photomicrograph of the interpleural space between the two lung lobules. Thickened pleura with extensive fibrin deposits is present on the left portion of the slide (1) and the right portion of the slide (2) contains the affected lung lobe. Note the extensive fibrin deposits in the interlobar space in the center portion of the slide (3).
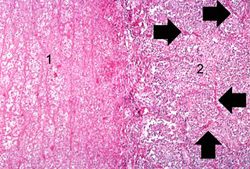
This photomicrograph of the lung shows the junction of the pleura (1) with the pneumonic lung parenchyma (2). Careful examination of the lung tissue at the right reveals the outline of alveolar structures in this tissue (arrows). The mass of cells infiltrating into this lung tissue consists almost exclusively of polymorphonuclear leukocytes (neutrophils).

This is another photomicrograph of the junction of the pleura (1) with the lung parenchyma. Note the alveoli on the left (2) filled with PMNs, alveolar macrophages, and fibrin. The dark red-stained material (3) in the center and left portions of the slide is fibrin in the pleura. There are red blood cells trapped in the fibrinous pleuritis as well.

This is a photomicrograph of alveoli filled with exudate. The alveolar wall outlines (arrows) are barely visible in this section. The alveoli are filled with PMNs, fibrin, and edema fluid. This is a severe acute inflammatory response but the structure of the alveoli remains intact. This tissue is able, with proper treatment, to completely resolve this inflammatory response. Since there has not been necrosis of the lung tissue itself (loss of tissue), this lung could completely recover normal function (resolution).








Virtual Microscopy[edit]
Lung: Lobar Pneumonia[edit]
Normal Lung[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Empyema and Abscess Pneumonia
- eMedicine Medical Library: Aspiration Pneumonia
- eMedicine Medical Library: Bacterial Pneumonia
- Merck Manual: Overview of Pneumonia
Journal Articles[edit]
- Domínguez J, Galí N, Matas L, Pedroso P, Blanco S, Giménez M, Prat C, Sopena N, Sabrià M, Ausina V. PCR detection of Streptococcus pneumoniae DNA in serum samples for pneumococcal pneumonia diagnosis. Clin Microbiol Infect 2001 Mar;7(3):164-6.
Images[edit]
Related IPLab Cases[edit]
A normal white blood cell count is 4,000 to 11,000 cells per cubic mm.
Nuchal rigidity is stiffness of the neck, a common sign of meningeal irritation.
CNS infections can lead to increased intracranial pressure, which, if severe, can cause death.
The normal weight of the right lung in an adult is 450 grams (range: 360 to 570 grams).
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.
An infiltrate is an accumulation of cells in the lung parenchyma--this is a sign of pneumonia.