IPLab:Lab 8:Hepatitis B
Contents
Clinical Summary[edit]
This was a 55-year-old white male with chronic renal failure who acquired hepatitis B virus (HBV) in a renal dialysis unit. Death was the result of multiple disease processes, which included active pulmonary tuberculosis and heart failure due to ischemic heart disease. There were few or no symptoms or signs of hepatitis during life other than seroconversion from negative to HBsAg positive.
At autopsy, the liver was enlarged due primarily to severe passive congestion.
Images[edit]

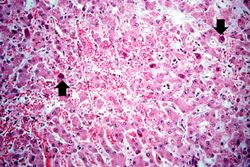
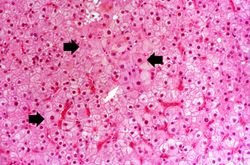
This is a low-power photomicrograph of liver from this case. This section was stained with a modified aldehyde fuchsin and counterstained with hematoxylin and eosin. Modified aldehyde fuchsin colors cystine-rich proteins--such as HBsAg and elastic fibers--deep purple. The cytoplasm of most liver cells (and RBCs) stain red due to the eosin and have dark blue nuclei.
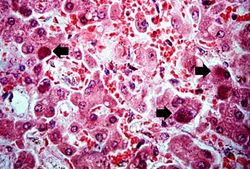
This is a higher-power photomicrograph of liver from this case. Note the severe congestion (RBCs in sinusoids) and the presence of occasional hepatocytes with dark red/magenta-stained cytoplasm (arrows).
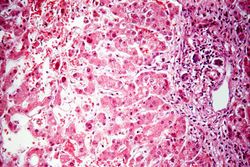
This is a higher-power photomicrograph of the periportal region exhibiting some inflammation and bile duct hyperplasia. There is also congestion and some loss of hepatocytes with disruption of the hepatic cords.
This is a high-power photomicrograph of liver with numerous hepatocytes containing accumulations of magenta-staining material in the cytoplasm (arrows).
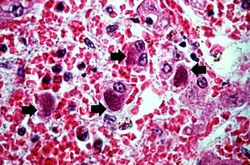
This high-power photomicrograph showing hepatocytes, the cytoplasm of which contain intracytoplasmic accumulations (arrows) of hepatitis B surface antigen.
This is a photomicrograph of a liver section from another case of hepatitis B. In this H&E-stained section, the typical "ground glass" appearance of the hepatocytes can be appreciated (arrows).

This is a low-power photomicrograph of liver from the previous image which has been reacted with antibody specific for HBsAg. The hepatocytes that contain HBsAg stain brown.
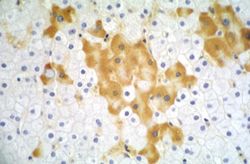
This higher-power photomicrograph of the previous section shows more clearly the HBsAg positive cells (arrows). Upon staining with H&E, these same cells exhibit a "ground glass" appearance, which is due to the accumulation of HBsAg in the hepatocyte cytoplasm.

This is a low-power photomicrograph of the same liver reacted with antibody specific for hepatitis B core antigen (HBcAg). The hepatocytes that contain HBcAg stain brown. Note that even at this low magnification, many brown-staining nuclei can be seen.
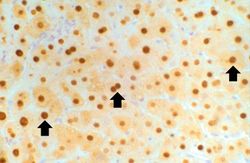
This high-power photomicrograph of the previous section shows the HBcAg positive nuclei (arrows).










Virtual Microscopy[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Hepatitis B
- Merck Manual: Acute Viral Hepatitis
- Merck Manual: Neonatal Hepatitis B Virus Infection
Journal Articles[edit]
- Merle P, Trepo C. Therapeutic management of hepatitis B-related cirrhosis. J Viral Hepat 2001 Nov;8(6):391-9.
Images[edit]
Related IPLab Cases[edit]
| |||||
Renal failure is the severe reduction of renal function and often leads to reduced urinary output.
Cirrhosis is a liver disease characterized by necrosis, fibrosis, loss of normal liver architecture, and hyperplastic nodules.
The normal fibrinogen level is 184 to 412 mg/dL.