IPLab:Lab 7:IDC
Contents
Clinical SummaryEdit
This 66-year-old female had had a mass of increasing size in the left breast for many years. A modified radical mastectomy was performed. At that time, invading carcinoma was left around the subclavian artery and 9 of 9 axillary lymph nodes were found to contain metastases. Later, pleural effusions recurred despite radiation therapy. The patient died 3 months after surgery.
At autopsy the left breast was large (1700 grams), measuring 34 x 22 x 7 cm. A very large tumor involving all quadrants and measuring about 14 cm in diameter was noted. The nipple and skin were involved, the latter showing the typical orange peel appearance. On section, virtually the entire breast was replaced by a tumor composed of firm, yellowish-white tissue. Extension into the fatty tissue and to the skin was evident grossly.
ImagesEdit
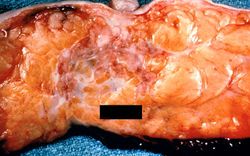
This is a gross photograph of the surgical specimen of breast with infiltrating duct carcinoma. Note the tumor tissue under the area of the nipple. The tumor infiltrates in an irregular fashion into the breast parenchyma. Note the nipple retraction caused by this neoplasm.

These are sections of normal breast (lower) and breast tissue with infiltrating duct carcinoma (upper). Note the increased cellularity (increased blue staining due to the increased number of nuclei) in the tumor tissue.
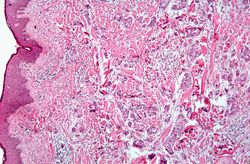
This is a section of breast with small groups of carcinoma cells throughout the breast tissue and invading through the dermis.
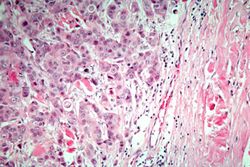
This is a higher-magnification showing abundant groups of tumor cells dissecting through the breast parenchyma - tumor infiltration (infiltrating duct cell carcinoma).
This is a high-power photomicrograph showing the cellular and nuclear features of the tumor cells. The large epithelial cells form glands and are medium-sized with a moderate amount of cytoplasm, vesicular nuclei, and nucleoli.
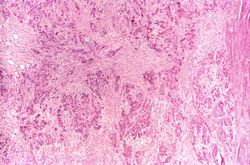
This is a section of breast tumor with abundant fibrous tissue throughout the tumor (desmoplasia, scirrhous carcinoma).
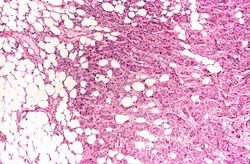
This is a section taken at the periphery of the tumor showing bands of tumor cells infiltrating into the fat tissue.
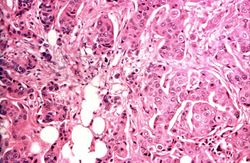
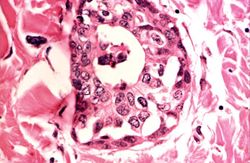
This is a high-power photomicrograph demonstrating the growth pattern of the tumor. The tumor consists of malignant duct-lining cells growing in cords, solid cell nests, tubules, and glands. The cytologic detail of tumor cells varies from small cells with moderately hyperchromatic, regular nuclei to large cells with large, irregular, hyperchromatic nuclei.








Virtual MicroscopyEdit
Study QuestionsEdit
Additional ResourcesEdit
ReferenceEdit
- eMedicine Medical Library: Breast Abscess and Masses
- eMedicine Medical Library: Breast Cancer
- Merck Manual: Breast Cancer
Journal ArticlesEdit
- Virnig BA, Tuttle TM, Shamliyan T, Kane RL. Ductal carcinoma in situ of the breast: a systematic review of incidence, treatment, and outcomes. J Natl Cancer Inst 2010 Feb 3;102(3):170-8.
ImagesEdit
Related IPLab CasesEdit
A radical mastectomy involves removal of the breast, underlying pectoralis muscles, and axillary lymph nodes.
Pleural effusion is the presence of fluid in the pleural space. Increased hydrostatic pressure in the pulmonary vasculature, as seen in heart failure, is one cause of pleural effusion.
An infiltrate is an accumulation of cells in the lung parenchyma--this is a sign of pneumonia.