Difference between revisions of "IPLab:Lab 4:Mural Thrombus"
Seung Park (talk | contribs) |
|||
| Line 17: | Line 17: | ||
File:IPLab4MuralThrombus7.jpg|This high-power photomicrograph of thrombus demonstrates more clearly the components of the layers--the pale regions which contain primarily platelets (degranulated platelets) with some fibrin (1), and the red areas which contain RBCs, some leukocytes, and fibrin (2). | File:IPLab4MuralThrombus7.jpg|This high-power photomicrograph of thrombus demonstrates more clearly the components of the layers--the pale regions which contain primarily platelets (degranulated platelets) with some fibrin (1), and the red areas which contain RBCs, some leukocytes, and fibrin (2). | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Study Questions == | ||
| + | * <spoiler text="Why do mural thrombi form on the endocardium of the heart after a myocardial infarction?">The infarct produced necrosis and inflammation. Also, the infarcted ventricular wall is akinetic and/or dyskinetic (bulges outward during systole). Thus, the blood in the ventricle tends to form thrombi on the surface of the infarcted endocardium.</spoiler> | ||
| + | * <spoiler text="List the sequence of events leading to mural thrombus formation.">* Platelets bind to damage endocardium and release ADP, 5-HT, thromboxane and platelet factor 4. | ||
| + | * This results in recruitment of more platelets and more degranulation of platelets with activation of the clotting cascade. | ||
| + | * Thrombin is activated leading to fibrin polymerization. | ||
| + | * This process results in the development of a platelet-fibrin thrombus.</spoiler> | ||
| + | * <spoiler text="What are possible sequelae of these mural thrombi?">The thrombotic material may break off and go to the brain or kidney (the two most likely sites since they get so much blood flow) or any arterial system.</spoiler> | ||
{{IPLab 4}} | {{IPLab 4}} | ||
[[Category: IPLab:Lab 4]] | [[Category: IPLab:Lab 4]] | ||
Revision as of 14:56, 21 August 2013
Clinical Summary[edit]
This 67-year-old female was transferred to the hospital from a nursing home in a comatose state. Physical findings on examination were compatible with brain stem infarction. On the fourth hospital day, an electrocardiogram revealed changes compatible with anterior myocardial infarction. The patient remained comatose with quadriplegia and expired on the 16th hospital day.
Autopsy Findings[edit]
Examination of the brain revealed extensive infarction involving the midbrain and cerebellum with complete occlusion of the upper one-half of the basilar artery; there was also extensive coronary artery atherosclerosis. A large aneurysm of the left ventricle was present; this was filled with mural thrombus. Extensive infarction of the lateral and posterior portions of the left ventricular wall toward the base of the heart was also found.
Images[edit]

This is a gross photograph of the heart from this case demonstrating the well-formed thrombus (arrow) tightly attached to the myocardium near the apex of the left ventricle.

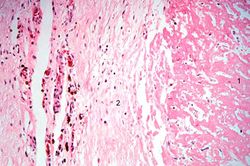
This is a low-power photomicrograph of the thrombus (1) attached to the myocardium (2).
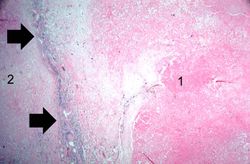
This higher-power photomicrograph shows the border between the thrombus on the right (1) and the endocardium on the left (2). There is a line of inflammatory cells at this interface (arrow).
This is a high-power photomicrograph of the border zone between the thrombus (1) and the endocardium (2). In this region there is less inflammation at the border zone.
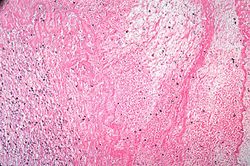
This photomicrograph illustrates the layered effect of the thrombus.
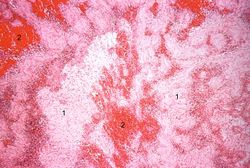
This is a higher-power photomicrograph of the thrombus. Note the pale regions which contain primarily platelets (degranulated platelets) with some fibrin (1), and the red areas which contain RBCs, some leukocytes, and fibrin(2).
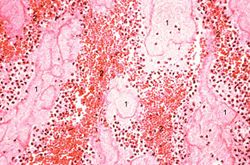
This high-power photomicrograph of thrombus demonstrates more clearly the components of the layers--the pale regions which contain primarily platelets (degranulated platelets) with some fibrin (1), and the red areas which contain RBCs, some leukocytes, and fibrin (2).







Study Questions[edit]
| |||||
Myocardial infarction is necrosis of myocardial tissue which occurs as a result of a deprivation of blood supply, and thus oxygen, to the heart tissue. Blockage of blood supply to the myocardium is caused by occlusion of a coronary artery.
An occlusion is a blockage.
Mural thrombosis is the formation of multiple thrombi along an injured endocardial wall.
A thrombus is a solid mass resulting from the aggregation of blood constituents within the vascular system.