Difference between revisions of "Cytologically Yours: CoW: 20131209"
(Created page with "== Clinical Summary == The patient is an 60 year old male with a remote history of an abdominal melanoma that was excised with negative margins. The patient has been experien...") |
(→Case Discussion) |
||
| (9 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| − | The patient is an | + | The patient is an 64 year old white male who presented with left sided back pain. Imaging showed a left perinephric retroperitoneal hematoma and a left renal lower pole cystic lesion with hemorrhage. Additional imaging showed numerous pulmonary lesions. An endobronchial ultrasound guided fine needle aspiration was scheduled. |
=== Past Medical History === | === Past Medical History === | ||
| − | * | + | * Congestive heart failure |
| − | * | + | * Ventricular tachycardia |
| − | * | + | * Ischemic heart disease |
=== Past Surgical History === | === Past Surgical History === | ||
| − | * | + | * Coronary stent placement |
| − | * | + | * Implant of AICD |
| − | |||
===Clinical Plan=== | ===Clinical Plan=== | ||
| − | The | + | The concern is a primary renal malignancy with metastatic disease to lungs. An endobronchial ultrasound guided FNA is scheduled. An onsite rapid diagnosis by cytology was scheduled. |
==Radiology== | ==Radiology== | ||
| − | * | + | * CT Abdomen shows a large perinephric hematoma and large low anterior structure in left lower pole suspicious for a hemorrhagic renal cell carcinoma. |
| − | * CT | + | * CT Chest shows multiple small lung lesions measuring up to 13x12 mm in greatest dimension. |
| + | ==Pathology== | ||
| + | ===Cytology=== | ||
| + | <gallery heights="250px" widths="250px"> | ||
| + | CytologicallyYoursCoW20131209Cytology1.jpg|4x magnification of a 4R lymph node. Groups of cohesive epithelial appearing cells can be seen on low power. Lymphoid tissue is not easily identified. | ||
| + | CytologicallyYoursCoW20131209Cytology2.jpg|20x magnification of a 4R lymph node. This is a cellular specimen with groups of cells along what appear to be a papillary or papillary-like structure. Single cells are also dispersed in the background. The cells are haphazardly arranged. | ||
| + | CytologicallyYoursCoW20131209Cytology3.jpg|40x magnification of a 4R lymph node. On higher power, the nuclei appear mildly atypical and the cytoplasm is delicate and finely vacuolated. The nuclear contours are somewhat irregular. | ||
| + | CytologicallyYoursCoW20131209Cytology4.jpg|Cell block of 4R lymph node. The cytoplasm does not appear as vacuolated on alcohol fixed cell block material, but the nuclei are relatively uniform, but somewhat atypical. | ||
| − | + | </gallery> | |
| − | === | + | ===Immunohistochemistry=== |
<gallery heights="250px" widths="250px"> | <gallery heights="250px" widths="250px"> | ||
| − | + | CytologicallyYoursCoW20131209Cytology5.jpg|PAX8 on 4R lymph node shows positive nuclear staining. | |
| − | |||
| − | |||
</gallery> | </gallery> | ||
====Resident Questions==== | ====Resident Questions==== | ||
| − | * <spoiler text="What | + | * <spoiler text="What are other immunohistochemical stains that would be applicable in this case?"> |
| − | * | + | * RCC |
| − | * | + | *CD10 |
| + | *PAX2 | ||
| + | *Kidney specific antigen | ||
| + | </spoiler> | ||
| + | |||
| − | <div class="usermessage mw-customtoggle-diagnosis" style="cursor:pointer">Click here to toggle the diagnosis | + | <div class="usermessage mw-customtoggle-diagnosis" style="cursor:pointer">Click here to toggle the diagnosis.</div> |
<div class="mw-collapsible mw-collapsed" id="mw-customcollapsible-diagnosis"> | <div class="mw-collapsible mw-collapsed" id="mw-customcollapsible-diagnosis"> | ||
<div class="mw-collapsible-content"> | <div class="mw-collapsible-content"> | ||
| Line 44: | Line 52: | ||
==Final Diagnosis== | ==Final Diagnosis== | ||
===Cytology=== | ===Cytology=== | ||
| − | * | + | * Rapid diagnosis: Non-small cell carcinoma. |
| + | * Final diagnosis: Renal cell carcinoma. | ||
| + | |||
| + | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
{{Cytologically Yours}} | {{Cytologically Yours}} | ||
[[Category:Case Reports]] | [[Category:Case Reports]] | ||
Latest revision as of 22:01, 15 January 2014
Contents
Clinical Summary
The patient is an 64 year old white male who presented with left sided back pain. Imaging showed a left perinephric retroperitoneal hematoma and a left renal lower pole cystic lesion with hemorrhage. Additional imaging showed numerous pulmonary lesions. An endobronchial ultrasound guided fine needle aspiration was scheduled.
Past Medical History
- Congestive heart failure
- Ventricular tachycardia
- Ischemic heart disease
Past Surgical History
- Coronary stent placement
- Implant of AICD
Clinical Plan
The concern is a primary renal malignancy with metastatic disease to lungs. An endobronchial ultrasound guided FNA is scheduled. An onsite rapid diagnosis by cytology was scheduled.
Radiology
- CT Abdomen shows a large perinephric hematoma and large low anterior structure in left lower pole suspicious for a hemorrhagic renal cell carcinoma.
- CT Chest shows multiple small lung lesions measuring up to 13x12 mm in greatest dimension.
Pathology
Cytology
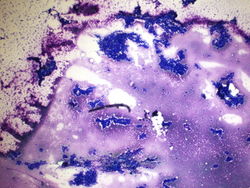
4x magnification of a 4R lymph node. Groups of cohesive epithelial appearing cells can be seen on low power. Lymphoid tissue is not easily identified.
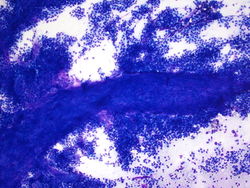
20x magnification of a 4R lymph node. This is a cellular specimen with groups of cells along what appear to be a papillary or papillary-like structure. Single cells are also dispersed in the background. The cells are haphazardly arranged.
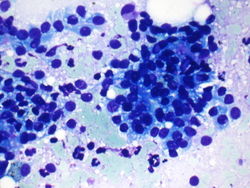
40x magnification of a 4R lymph node. On higher power, the nuclei appear mildly atypical and the cytoplasm is delicate and finely vacuolated. The nuclear contours are somewhat irregular.
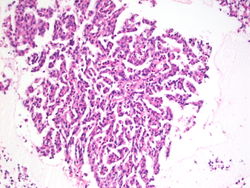
Cell block of 4R lymph node. The cytoplasm does not appear as vacuolated on alcohol fixed cell block material, but the nuclei are relatively uniform, but somewhat atypical.




Immunohistochemistry
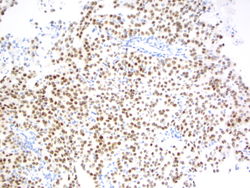
PAX8 on 4R lymph node shows positive nuclear staining.

Resident Questions
Final Diagnosis
Cytology
- Rapid diagnosis: Non-small cell carcinoma.
- Final diagnosis: Renal cell carcinoma.
| ||||||||