Difference between revisions of "Cytologically Yours: CoW: 20131202"
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| − | The patient is an | + | The patient is an 60 year old male with a remote history of an abdominal melanoma that was excised with negative margins. The patient has been experiencing lower back pain for the past several months and has received epidural injections. As a part of the workup, the patient had a CT which revealed retroperitoneal lymphadenopathy. A CT guided fine needle aspiration and biopsy of a paracaval lymph node was performed. |
=== Past Medical History === | === Past Medical History === | ||
| − | * | + | * 2003 Melanoma |
| − | * | + | * Diabetes |
* Hypertension | * Hypertension | ||
| − | |||
| − | |||
| − | |||
| − | |||
=== Past Surgical History === | === Past Surgical History === | ||
| − | * | + | * 2013 Arthroscopic knee surgery |
| − | * | + | * 2003 Excision of melanoma |
| − | * | + | * 2002 Discectomy |
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
===Clinical Plan=== | ===Clinical Plan=== | ||
| − | + | The differential diagnosis for otherwise asymptomatic lymphadenopathy in this patient is melanoma, lymphoma, or occult malignancy. | |
==Radiology== | ==Radiology== | ||
| − | CT | + | * PET CT showed hypermetabolic activity with an SUV of 12.7. |
| − | + | * CT of abdomen and pelvis showed adenopathy adjacent to the aorta and inferior to the vena cava at the level of the right kidney. The largest node measured 4 cm in greatest dimension. | |
| − | |||
===CT=== | ===CT=== | ||
| Line 54: | Line 38: | ||
====Resident Questions==== | ====Resident Questions==== | ||
| − | * <spoiler text=" | + | * <spoiler text="What is your differential diagnosis?">These groups of cells demonstrate malignant appearing cells in a background of an otherwise benign appearing lymphoid background. The atypical cells are scattered, with large nucleoli and several binucleate forms. In addition, there seem to be an increased number of eosinophils in the background. The differential diagnosis includes Hodgkin lymphoma; however, the possibility of the large atypical cells being melanoma cannot be ruled out. </spoiler> |
* <spoiler text="What would you call this on a Rapid Interpretation?">This is a male patient with no previous history of malignancy. Our differential diagnosis can include many entities. However, these are cohesive cells so lymphoma should be at the bottom of our list. We would need more information to classify these cells, but a diagnosis of positive for malignancy (with no further specificity) can be rendered.</spoiler> | * <spoiler text="What would you call this on a Rapid Interpretation?">This is a male patient with no previous history of malignancy. Our differential diagnosis can include many entities. However, these are cohesive cells so lymphoma should be at the bottom of our list. We would need more information to classify these cells, but a diagnosis of positive for malignancy (with no further specificity) can be rendered.</spoiler> | ||
Revision as of 20:01, 14 January 2014
Contents
Clinical Summary
The patient is an 60 year old male with a remote history of an abdominal melanoma that was excised with negative margins. The patient has been experiencing lower back pain for the past several months and has received epidural injections. As a part of the workup, the patient had a CT which revealed retroperitoneal lymphadenopathy. A CT guided fine needle aspiration and biopsy of a paracaval lymph node was performed.
Past Medical History
- 2003 Melanoma
- Diabetes
- Hypertension
Past Surgical History
- 2013 Arthroscopic knee surgery
- 2003 Excision of melanoma
- 2002 Discectomy
Clinical Plan
The differential diagnosis for otherwise asymptomatic lymphadenopathy in this patient is melanoma, lymphoma, or occult malignancy.
Radiology
- PET CT showed hypermetabolic activity with an SUV of 12.7.
- CT of abdomen and pelvis showed adenopathy adjacent to the aorta and inferior to the vena cava at the level of the right kidney. The largest node measured 4 cm in greatest dimension.
CT



Pathology
Cytology
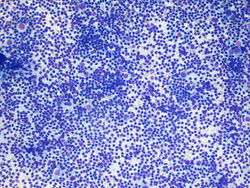
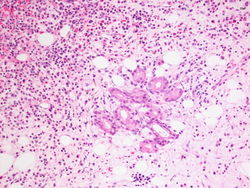
10x magnification of paracaval lymph node. There is a polymorphic lymphoid population with scattered large atypical cells.
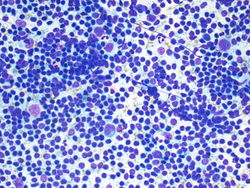
20x magnification of paracaval lymph node. There are small lymphocytes with background lymphoglandular bodies. Scattered eosinophils and large atypical cells with prominent nucleoli.
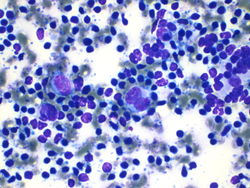
40x magnification of paracaval lymph node. There are atypical binucleated cells among the large atypical cells.



Resident Questions
Biopsy
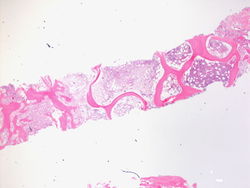
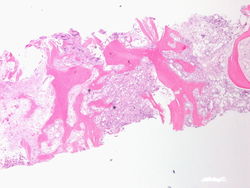
This is a 2x magnification the biopsy specimen from the spinal mass. We see that this is bone histology which is abnormal. There is an increase in cellularity, especially for an 80 year old person.
This is a 4x magnification of the biopsy specimen from the spinal mass. We can see that there is an increase in cellularity.
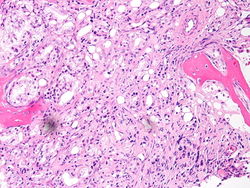
This is a 20x magnification of the biopsy specimen from the spinal mass. This is one of the areas that has increased cellularity on lower power. We can see cells forming what appear to be glands in the bone marrow.
This is a 20x magnification of the biopsy specimen from the spinal mass. Here we see well formed glands in the bone marrow.
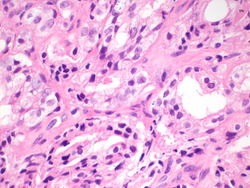
This is a 60x magnification of the biopsy specimen from the spinal mass. The malignant cells appear to be creating glandular structures, and we can identify prominent nucleoli in the malignant cells.
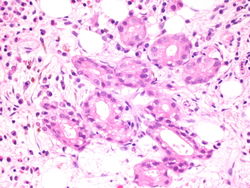
This is a 60x magnification of the biopsy specimen from the spinal mass. Again we see well formed glands in the bone marrow, made of cells that have prominent nucleoli.






Immunohistochemistry
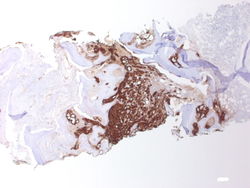
PSA, 2x magnification. Note the predominance of brown staining in the middle.
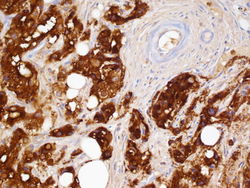
PSA, 60x magnification. The glands are highlighted in brown, and on the upper right the blood vessels are negative.


Resident Questions
Final Diagnosis
Cytology
- Positive for malignancy.
Biopsy
- Metastatic prostatic adenocarcinoma.
Case Discussion
This is a classic case of prostatic adenocarcinoma, metastatic to the spine.
| ||||||||