Difference between revisions of "Cytologically Yours: CoW: 20131125"
(No difference)
|
Revision as of 23:05, 19 November 2013
Contents
Clinical History
45 year old woman who presented to her primary care physician with fever for 5 months (Tmax of 102F), night sweats, and neck pain. She stated that she had pain with swallowing and felt as though her heart was racing. She denies any other associated symptoms.
Past Medical History
No medical problems
Procedures and Past Surgical History
- Upper endoscopy
- Appendectomy
- Vaginal delivery
Allergies and Medications
- Allergy to penicillin (rash)
- Hydroxyzine
- Omeprazole
- Fenofenadine
Physical Exam
- Temperature: 98.5 F
- Blood Pressure: 90/60
- Heart Rate: 102bpm
- Weight: 43.27 kg
- Height: 62.5 inches
- Neck: Mild sub-maxillary and anterior cervical lymphadenopathy. In the left thyroid lobe a 1.0 x 0.5cm mass was palpated. This nodule was tender to touch and did not have any associated erythema.
- The remainder of the exam was within normal limits.
Radiology
Ultrasound
- Right lobe measured 4.5 x 1.5 x 1.3cm. Multiple nodules were identified in the right lobe and the largest measured 2.0 x 1.5 x 0.7cm.
- Left lobe measured 4.6 x 2.0 x 1.1cm. This lobe was largely replaced by a single nodule measuring 3.3 x 2.1 x 2.0cm.
Management
The patient is sent home with instructions to follow up in a week.
Follow Up Appointment
One week later the patient returns and complains of continued fever and night sweats.
Lab Results
- Free T4 2.62 mg/dL (normal range 0.62-1.57 mg/dL)
- TSH 0.035 mcIntUnits/mL (normal range 0.350-5.500 mcIntUnits/mL)
- Anti-TPO <63 units (normal is <100 units)
- An uptake scan is performed, and shows decreased uptake in the presence of hyperthyroidism. This is called consistent with subacute thyroiditis.
Plan
Repeat thyroid function tests and biopsy the large nodule in the left lobe with the labs normalize.
Pathology
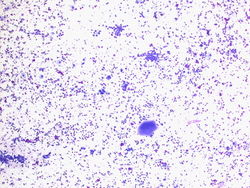
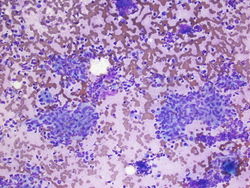
4x magnification of the specimen. We see colloid, few small clusters of cells macrophages, and scattered cells in the background.
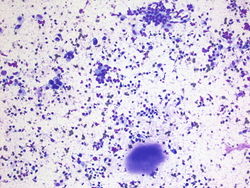
20x magnification. Colloid is present at the bottom of the field. There are single cells in the background and small groups of cells.
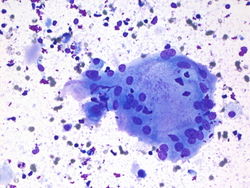
40x magnification of a large multinucleated giant cell. There is colloid and macrophages present in the background.
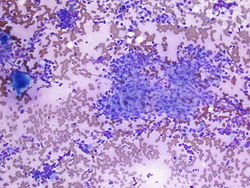
10x magnification. Here we have a large cohesive group of spindled epithelioid cells. The centers are non-necrotizing. In the background there is colloid and single cells present.
10x magnification. Here there are more groups of cohesive epithleioid spindled cells with non-necrotizing centers.
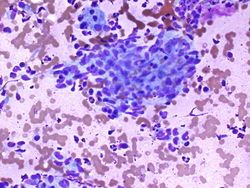
40x magnification of a group of cohesive epithelioid spindled cells with non-necrotizing center.






Resident Questions
Diagnosis
Cytology
Benign aspirate, see comment.
COMMENT: There are non-necrotizing granulomas, benign follicular cells, macrophages, colloid, lymphocytes, and multinucleated giant cells; consistent with granulomatous thyroiditis.
Case Discussion
Granulomatous Thyroiditis is also known as deQuervain or subacute thyroiditis. It is a postviral syndrome. Usual presentation is in a young woman who has just gotten over a cold.
Patients present with painful thyroid, fever, fatigue, chills. Diagnosis is usually made clinically, therefore FNA biopsy is usually not performed. The disease is usually self-limiting.
If an aspirate is performed it may be scantly cellular due to pain and fibrosis. If material is gathered you may see non-caseating granulomas, colloid, chronic inflammation, and multinucleated giant cells.
| ||||||||