IPLab:Lab 10:Candidiasis
Contents
Clinical Summary[edit]
This 73-year-old black male was in good health until about three months before his death when he noticed enlarged lymph nodes first in both inguinal regions and later elsewhere. Antileukemic therapy was begun. About two weeks prior to his death the patient presented to the emergency room with uncontrollable epistaxis. On physical examination, the liver was palpable but the spleen was not. The white blood count was below normal and consisted mainly of lymphocytes with many atypical cells. The patient's bone marrow was also found to be heavily loaded with lymphocytes. Platelets were extremely low and remained so despite platelet transfusions. Subsequently, the patient developed pneumonia which progressed until death. Antemortem cultures yielded Candida tropicalis and Pseudomonas aeruginosa.
Autopsy Findings[edit]
At autopsy, there was evidence of disseminated candidiasis.
Images[edit]

This autopsy photograph of the kidneys demonstrates the multifocal punctate lesions visible on the serosal surface (arrows). Don't confuse these small yellow punctate lesions with the fat that is adherent to the renal capsule.

This photograph of the cut surface of these kidneys shows that these multifocal punctate lesions are primarily in the cortex (arrows).
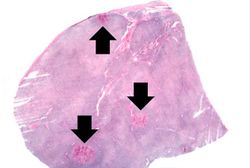
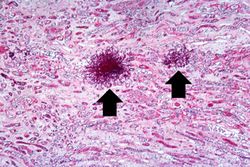
This is a low-power photomicrograph of lymph node with three prominent areas of Candida colonies (arrows). Even at this low magnification, the purple-staining yeast and pseudohyphae can be easily seen. This section was stained with Periodic Acid-Schiff Hematoxylin (PASH ), which stains the cell wall of fungi to make them more easily visible.
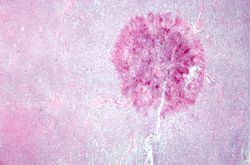
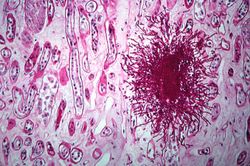
This is a low-power photomicrograph of one of the Candida colonies from this lymph node. The chains of yeast which are termed "pseudohyphae" are apparent at this magnification.
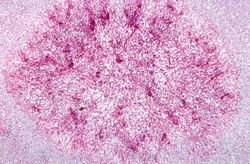
This higher-power photomicrograph shows the yeasts and pseudohyphae in this focus of Candida organisms.
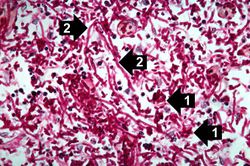
This high-power photomicrograph shows the yeasts (1) and pseudohyphae (2).
This is a low-power photomicrograph of the kidney from this same case. Note the Candida colonies (arrows). The pseudohyphae are evident around the periphery of these colonies even at this low magnification.
This is a higher-power photomicrograph of a Candida colony in the kidney. Note the pseudohyphae of the Candida organisms.








Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Candidiasis in Emergency Medicine
- eMedicine Medical Library: Candidiasis
- Merck Manual: Candidiasis (Invasive)
Journal Articles[edit]
Images[edit]
Related IPLab Cases[edit]
| |||||
Epistaxis is bleeding from the nose.
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.