Difference between revisions of "Cytologically Yours: CoW: 20131216"
| (8 intermediate revisions by the same user not shown) | |||
| Line 22: | Line 22: | ||
===Cytology=== | ===Cytology=== | ||
<gallery heights="250px" widths="250px"> | <gallery heights="250px" widths="250px"> | ||
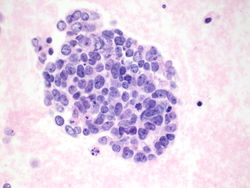
| − | CytologicallyYoursCoW20131216Cytology1.jpg| | + | CytologicallyYoursCoW20131216Cytology1.jpg|10x magnification of pleural fluid(ThinPrep). Groups of cohesive epithelial appearing cells are seen on low power. |
| − | CytologicallyYoursCoW20131216Cytology2.jpg| | + | CytologicallyYoursCoW20131216Cytology2.jpg|40x magnification of pleural fluid (ThinPrep). Cluster of atypical cells showing nuclear pleomorphism and scant cytoplasm. |
| − | CytologicallyYoursCoW20131216Cytology3.jpg|40x magnification of | + | CytologicallyYoursCoW20131216Cytology3.jpg|40x magnification of pleural fluid (ThinPrep). Chromatin is irregular and clumped with salt and pepper appearance; although, occasional nucleoli are also seen. |
| − | CytologicallyYoursCoW20131216Cytology4.jpg| | + | CytologicallyYoursCoW20131216Cytology4.jpg|40x magnification of pleural fluid (ThinPrep). Some nuclear molding can be appreciated and a mitotic figure is present. |
| − | CytologicallyYoursCoW20131216Cytology5.jpg|Cell block of | + | CytologicallyYoursCoW20131216Cytology5.jpg|Cell block of pleural fluid. Group of malignant cells showing nuclear molding, scant cytoplasm, and salt and pepper chromatin. Nucleoli are also seen. |
| Line 38: | Line 38: | ||
</gallery> | </gallery> | ||
| − | ==== | + | ====Other immunostains performed==== |
| − | * | + | * BerEp4 Positive |
| − | * | + | * Moc31 Faintly positive |
| − | * | + | * Calretinin Negative |
| − | * | + | * TTF1 Negative |
| − | * | + | * Chromogranin Positive |
| − | + | * Synaptophysin Positive | |
| + | * CD56 Positive | ||
| + | * Napsin A Negative | ||
| − | + | <div class="usermessage mw-customtoggle-diagnosis" style="cursor:pointer">Click here to toggle the diagnosis.</div> | |
| − | |||
| − | <div class="usermessage mw-customtoggle-diagnosis" style="cursor:pointer">Click here to toggle the diagnosis | ||
<div class="mw-collapsible mw-collapsed" id="mw-customcollapsible-diagnosis"> | <div class="mw-collapsible mw-collapsed" id="mw-customcollapsible-diagnosis"> | ||
<div class="mw-collapsible-content"> | <div class="mw-collapsible-content"> | ||
| Line 55: | Line 55: | ||
==Final Diagnosis== | ==Final Diagnosis== | ||
===Cytology=== | ===Cytology=== | ||
| − | * | + | * Small cell carcinoma |
| − | |||
| − | |||
| + | ===Discussion=== | ||
| + | The differential diagnosis includes large cell neuroendocrine carcinoma, and possibly nonkeratinizing squamous cell carcinoma and adenocarcinoma. In this case, we know that we are dealing with a poorly differentiated neuroendocrine carcinoma based on immunohistochemistry. In addition, except for the occasional nucleoli, this lesion has all of the features of a small cell carcinoma (scant cytoplasm, nuclear molding). In this case, the possibility of a poorly differentiated carcinoma with mixed large cell and small cell features may not be able to be completely ruled out on cytology of the pleural fluid. It has been determined that prominent nucleoli may be seen in small cell carcinomas up to 24% of the time (Khalbuss WE The cytomorphologic spectrum of small-cell carcinoma and large-cell neuroendocrine carcinoma in body cavity effusions: A study of 68 cases. CytoJournal 2011, 8:18. [[http://www.cytojournal.com/article.asp?issn=1742-6413;year=2011;volume=8;issue=1;spage=18;epage=18;aulast=Khalbuss]] | ||
| − | |||
| − | |||
</div></div> | </div></div> | ||
Latest revision as of 22:03, 15 January 2014
Contents
Clinical Summary
The patient is an 66 year old white male with a history of smoking, COPD, and diabetes. The patient presented with increased shortness of breath.
Past Medical History
- Diabetes
- COPD
- Squamous cell carcinoma of skin
Past Surgical History
- Excision of squamous cell carcinoma
- Removal of adenomatous polyp of sigmoid colon
Clinical Plan
The differential diagnosis includes worsening of COPD. CT imaging of chest is performed.
Radiology
- CT Chest shows hilar lung mass and multiple mediastinal lymph nodes showing increased uptake on PET scan.
Pathology
Cytology
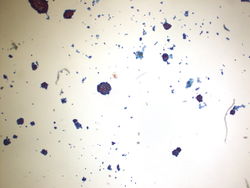
10x magnification of pleural fluid(ThinPrep). Groups of cohesive epithelial appearing cells are seen on low power.
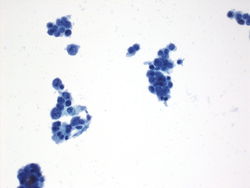
40x magnification of pleural fluid (ThinPrep). Cluster of atypical cells showing nuclear pleomorphism and scant cytoplasm.
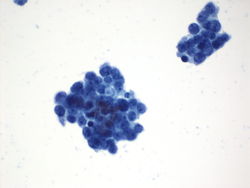
40x magnification of pleural fluid (ThinPrep). Chromatin is irregular and clumped with salt and pepper appearance; although, occasional nucleoli are also seen.
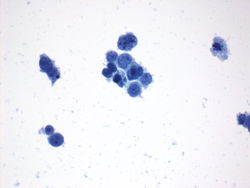
40x magnification of pleural fluid (ThinPrep). Some nuclear molding can be appreciated and a mitotic figure is present.
Cell block of pleural fluid. Group of malignant cells showing nuclear molding, scant cytoplasm, and salt and pepper chromatin. Nucleoli are also seen.





Immunohistochemistry
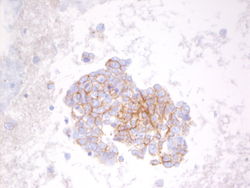
CD56 on pleural fluid shows positive cytoplasmic staining.
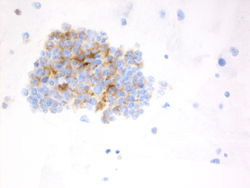
Synaptophysin on pleural fluid shows positive cytoplasmic staining.


Other immunostains performed
- BerEp4 Positive
- Moc31 Faintly positive
- Calretinin Negative
- TTF1 Negative
- Chromogranin Positive
- Synaptophysin Positive
- CD56 Positive
- Napsin A Negative
Final Diagnosis
Cytology
- Small cell carcinoma
Discussion
The differential diagnosis includes large cell neuroendocrine carcinoma, and possibly nonkeratinizing squamous cell carcinoma and adenocarcinoma. In this case, we know that we are dealing with a poorly differentiated neuroendocrine carcinoma based on immunohistochemistry. In addition, except for the occasional nucleoli, this lesion has all of the features of a small cell carcinoma (scant cytoplasm, nuclear molding). In this case, the possibility of a poorly differentiated carcinoma with mixed large cell and small cell features may not be able to be completely ruled out on cytology of the pleural fluid. It has been determined that prominent nucleoli may be seen in small cell carcinomas up to 24% of the time (Khalbuss WE The cytomorphologic spectrum of small-cell carcinoma and large-cell neuroendocrine carcinoma in body cavity effusions: A study of 68 cases. CytoJournal 2011, 8:18. [[1]]
| ||||||||