IPLab:Lab 6:Hashimoto's Thyroiditis
Contents
Clinical SummaryEdit
This was a 49-year-old woman who complained of tiredness and difficulty concentrating. She had gained weight over the last year and despite warm weather, she felt chilled without a sweater. Family history was significant for hypothyroidism in her mother and older sister.
On physical examination she had an enlarged thyroid gland with a firm, bosselated texture. Serum TSH was markedly elevated and antithyroid peroxidase antibodies were positive. These results supported the clinical impression of hypothyroidism; also, the texture of her thyroid gland and a positive family history suggested an autoimmune etiological factor. She was referred to an endocrinologist; however, before beginning treatment she died suddenly from a ruptured berry aneurysm.
Autopsy FindingsEdit
At autopsy, significant subarachnoid hemorrhage from the ruptured berry aneurysm was documented. In addition, the thyroid gland was mildly enlarged and firm. On cut section the tissue was slightly pale.
ImagesEdit

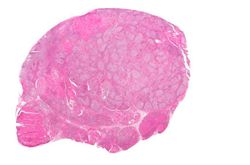
This is a gross photograph of thyroid gland taken at autopsy. The gland is only slightly enlarged and has a firm texture.
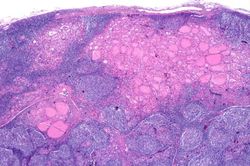
This is a low-power photomicrograph of thyroid from this case. Note that the tissue is more cellular than one would expect and there does not appear to be normal colloid-filled blue spaces in this gland.
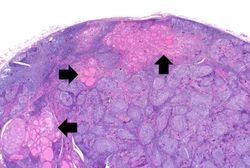
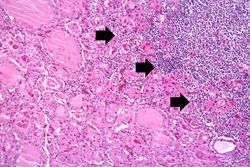
This is a higher-power photomicrograph of thyroid from this case. Note the large number of blue-staining inflammatory cells in this tissue. These cells appear to be forming germinal centers. Some residual thyroid gland tissue can be seen in this section (arrows).
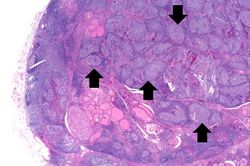
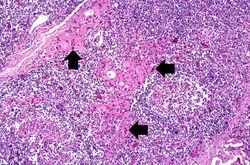
This is another view of thyroid gland filled with inflammatory cells forming germinal centers (arrows).
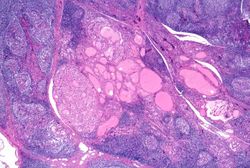
This is a higher-power photomicrograph of thyroid from this case showing the inflammatory cells and the residual thyroid tissue.
This is another higher-power photomicrograph of thyroid from this case showing the inflammatory cells and the residual thyroid tissue.
This is a high-power photomicrograph showing the inflammatory cells infiltrating into the residual thyroid tissue (arrows).
This is a high-power photomicrograph showing the lymphocytes and plasma cells surrounding the thyroid gland epithelium.
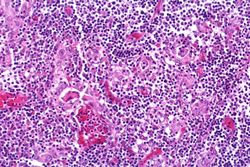
This high-power photomicrograph shows more clearly the lymphocytes and plasma cells surrounding the thyroid gland epithelium. Large, eosinophilic, degenerating thyroid gland cells (Hurthle cells) can be seen in this section (arrows).
Virtual MicroscopyEdit
Study QuestionsEdit
Additional ResourcesEdit
ReferenceEdit
- eMedicine Medical Library: Hashimoto Thyroiditis
- eMedicine Medical Library: Hypothyroidism
- Merck Manual: Overview of Thyroid Function
- Merck Manual: Hashimoto's Thyroiditis
- Merck Manual: Hypothyroidism
Journal ArticlesEdit
- Agrawal P, Ogilvy-Stuart A, Lees C. Intrauterine diagnosis and management of congenital goitrous hypothyroidism. Ultrasound Obstet Gynecol 2002 May;19(5):501-5.
ImagesEdit
Related IPLab CasesEdit
Bosselated means covered with rounded protuberances.
Autoimmune disorders involve an immune response directed at the host's own cells.
A berry aneurysm is a small saccular arterial aneurysm usually found at a vessel junction in the circle of Willis. These aneurysms frequently rupture, causing a subarachnoid hemorrhage.