Difference between revisions of "IPLab:Lab 4:Chronic Passive Congestion"
Seung Park (talk | contribs) (→Images) |
(→Autopsy Findings) |
||
| (4 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| + | This 57-year-old male was hospitalized with a three-month history of a dry, hacking cough, dyspnea, and chest pain. He was diagnosed as having congestive heart failure. There was no evidence of myocardial infarction, but renal and hepatic functions were decreased. The patient developed refractory congestive heart failure and renal failure. The patient's cardiac index was marginal and he was classified as a having congestive cardiomyopathy. The patient had a cardiorespiratory arrest and died two months after admission. | ||
| − | + | At autopsy the lungs were congested and edematous with evidence of lobar pneumonia. The heart weighed 540 grams and showed 75 to 95% atherosclerotic stenosis of all the major coronary arteries. The right and left ventricles were markedly dilated. The ventricular walls were extremely thin with patchy areas of subendocardial fibrosis. The liver weighed 1630 grams and displayed the classic "nutmeg appearance" of chronic passive hepatic congestion on cut surface. | |
| − | |||
| − | |||
| − | |||
| − | At autopsy the lungs were congested and edematous with evidence of lobar pneumonia. The heart weighed 540 grams and showed 75 to 95% atherosclerotic stenosis of all the major coronary arteries. The right and left ventricles were markedly dilated. The ventricular walls were extremely thin with patchy areas of subendocardial fibrosis. The liver weighed 1630 grams and displayed the classic "nutmeg appearance" of chronic passive hepatic congestion on cut surface. | ||
== Images == | == Images == | ||
| Line 19: | Line 16: | ||
File:IPLab4ChronicPassiveCongestion9.jpg|This is a gross photograph of the cut surface of a liver with chronic passive congestion (left) compared to the cut surface of a nutmeg (right). | File:IPLab4ChronicPassiveCongestion9.jpg|This is a gross photograph of the cut surface of a liver with chronic passive congestion (left) compared to the cut surface of a nutmeg (right). | ||
</gallery> | </gallery> | ||
| + | |||
| + | == Virtual Microscopy == | ||
| + | === Liver Chronic Passive Congestion === | ||
| + | <peir-vm>IPLab4ChronicPassiveCongestion</peir-vm> | ||
| + | |||
| + | === Normal Liver === | ||
| + | <peir-vm>UAB-Histology-00149</peir-vm> | ||
== Study Questions == | == Study Questions == | ||
Latest revision as of 01:56, 24 June 2020
Contents
Clinical SummaryEdit
This 57-year-old male was hospitalized with a three-month history of a dry, hacking cough, dyspnea, and chest pain. He was diagnosed as having congestive heart failure. There was no evidence of myocardial infarction, but renal and hepatic functions were decreased. The patient developed refractory congestive heart failure and renal failure. The patient's cardiac index was marginal and he was classified as a having congestive cardiomyopathy. The patient had a cardiorespiratory arrest and died two months after admission.
At autopsy the lungs were congested and edematous with evidence of lobar pneumonia. The heart weighed 540 grams and showed 75 to 95% atherosclerotic stenosis of all the major coronary arteries. The right and left ventricles were markedly dilated. The ventricular walls were extremely thin with patchy areas of subendocardial fibrosis. The liver weighed 1630 grams and displayed the classic "nutmeg appearance" of chronic passive hepatic congestion on cut surface.
ImagesEdit

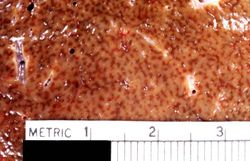
This is a gross photograph of a liver demonstrating chronic passive congestion. Note the accentuation of the centrilobular pattern evidenced by the dark-brown-staining areas in this tissue.
This is a closer view of a cut section of liver demonstrating the pattern of chronic passive congestion. The central vein regions are red and the surrounding hepatic tissue is pale tan-brown.
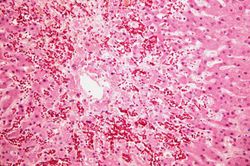
This low-power photomicrograph of liver demonstrates a slightly visible pattern of centrilobular congestion at this magnification.
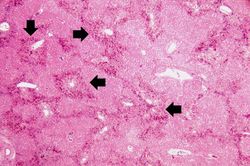
This is a higher-power photomicrograph of liver demonstrating an accentuated lobular pattern with a dark red stain surrounding the central veins in the liver lobules (arrows).
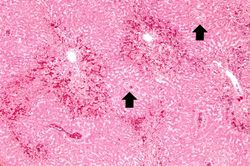
This higher-power photomicrograph of the liver lobules shows congestion and red blood cell accumulation in the sinusoidal spaces around the central vein. Note that around the portal triads (arrows) the liver cells are quite normal and there is no evidence of congestion.
This is a high-power photomicrograph of the central vein illustrating congestion and some loss of liver parenchymal cells. A mild increase in connective tissue around the central vein is evident in this section.
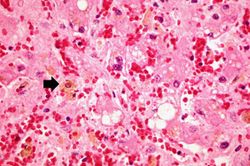
This is a high-power photomicrograph of liver with several macrophages that are distended with a brown pigment (arrow). These resident macrophages (Kupffer cells) are part of the reticuloendothelial system and normally line the sinusoidal spaces in the liver where they phagocytose the RBCs that pool, and eventually die, in the central vein region.

This is a gross photograph of a nutmeg. You can see from the appearance of the cut surface of the nutmeg (arrow) why chronic passive congestion of the liver is sometimes referred to as "nutmeg liver."

This is a gross photograph of the cut surface of a liver with chronic passive congestion (left) compared to the cut surface of a nutmeg (right).









Virtual MicroscopyEdit
Study QuestionsEdit
Additional ResourcesEdit
ReferenceEdit
- eMedicine Medical Library: Cardiac Cirrhosis and Congestive Hepatopathy
- eMedicine Medical Library: Myocarditis
- eMedicine Medical Library: Pediatric Congestive Heart Failure
- Merck Manual: Cirrhosis
Journal ArticlesEdit
- Naschitz JE, Slobodin G, Lewis RJ, Zuckerman E, Yeshurun D. Heart diseases affecting the liver and liver diseases affecting the heart. Am Heart J 2000 Jul;140(1):111-20.
ImagesEdit
Related IPLab CasesEdit
Myocardial infarction is necrosis of myocardial tissue which occurs as a result of a deprivation of blood supply, and thus oxygen, to the heart tissue. Blockage of blood supply to the myocardium is caused by occlusion of a coronary artery.
Renal failure is the severe reduction of renal function and often leads to reduced urinary output.
Cardiac index is a measure of a patient's cardiac output in relation to body size.
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.
A normal heart weighs 300 grams (range: 270 to 360 grams).
A normal liver weighs 1650 grams (range: 1500 to 1800 grams).
Chronic passive hepatic congestion is a disorder seen in conjunction with right-sided heart failure. In right-sided heart failure, peripheral venous pressures increase and thus reduce outflow from the liver. The result is a chronically congested liver.