){kind=link}
){kind=link}

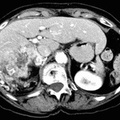
RADIOLOGY: KIDNEY: Case# 32984: RENAL CELL CA - EXTREMELY VASCULAR. 74 year old woman with history of renal mass seen on outside study. This study is done for staging. There is a hiatal hernia present. There is a large heterogeneous mass that enhances brightly replacing most of the right kidney. Overall, the mass measures approximately 11cm AP by 7cm transverse by 12cm cranio-caudal. There is a thin rim of preserved renal parenchyma inferiorly, with hydronephrosis of the adjacent collecting system. There are numerous collateral vessels surrounding the periphery of this large mass. The mass causes an impression on the inferior aspect of the liver and also displaces the head and neck of the pancreas anteriorly. Invasion into either of these organs cannot be excluded. The right renal vein is not identified. There is adenopathy posterior to the inferior vena cava, measuring approximately 1.8cm x 1.6cm. There is no evidence of extension of mass into the inferior vena cava. There is diverticulosis in the sigmoid colon. 85% of renal neoplasms are renal cell carcinomas, most commonly occurring in men, at ages 50-70, and usually involving one kidney. Only 2% are bilateral. Metastases are present at the time of diagnosis in 40% of cases. Since surgery is the only cure, early detection and accurate staging are important. The most common CT finding is a solid mass although low density areas due to hemorrhage or necrosis may be present. Cystic and multicystic forms may be seen. Stippled central or "eggshell" peripheral calcifications are seen in 10%. These tumors are usually hypervascular which may be evidenced by the presence of tortuous vessels in the perirenal fat. Tumor growth into the renal vein occurs in 30% of the time and into the inferior vena cava 5-10%. Venous invasion does not preclude surgical resection, but its identification is crucial to surgical planning. Renal cell carcinomas may spread locally to perirenal fat and adjacent organs. This is seen as strand or nodules of low density. Enlargement of renal hilar, pericaval, and periaortic nodes to 15mm or more indicates lymphatic spread. Hematogenous spread to the lung, bone, liver, adrenals, and the opposite kidney may occur. Distant metastases occasionally disappear with the removal of the primary tumor. Late appearance of metastases as long as 20 years following "cure" is also seen.

- Author
- Peter Anderson
- Posted on
- Thursday 1 August 2013
- Tags
- adrenal hemorrhage, kidney, radiology
- Albums
- Visits
- 2044
0 comments