){kind=link}
){kind=link}

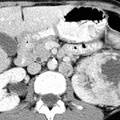
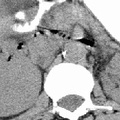
RADIOLOGY: KIDNEY: Case# 32913: L. RENAL MASS W/ LOCAL NODES, RENAL CELL ADENO. 45 year old female with hematuria. Comparison is made to a prior abdominal CT. The large, heterogeneous, enhancing left renal mass is again seen. It now measures 6.6 x 7.9cm and previously measured 6 x 6.5cm. Pre contrast images through this region show a small area of higher attenuation in the posteromedial portion of this mass. The right kidney, ureters, and bladder are radiographically unremarkable. Nodular enlargement is again seen in the right adrenal gland. This area measures 0.8 x 1.2cm in diameter. It is better visualized on todays examination and shows some areas of enhancement. The left adrenal gland is slightly prominent, but its adeniform contour is preserved. The renal vein is prominent but appears patent as do the other major vessels in the upper abdomen. 85% of renal neoplasms are renal cell carcinomas. They most commonly occur in men, at ages 50-70, and are usually unilateral. Only 2% are bilateral. Metastases are present at the time of diagnosis in 40% of cases. Since surgery is the only cure, early detection and accurate staging are important. Contrast-enhanced CT detects 96% of renal cell carcinomas. When IV contrast administration is contraindicated, MR is the preferred method of evaluation. The most common CT finding is a solid mass although low density areas due to hemorrhage or necrosis may be present. Strongly enhancing tumors are lower in density than renal parenchyma. Cystic and multicystic forms may be seen. Stippled central or "eggshell" peripheral calcifications are seen in 10%. These tumors are usually hypervascular which may be evidenced by the presence of tortuous vessels in the perirenal fat. Tumor growth into the renal vein occurs in 30% of the time and into the inferior vena cava 5-10%. Venous invasion does not preclude surgical resection, but its identification is crucial to surgical planning. CT typically shows enlarged, poorly enhancing veins which are filled with tumor thrombus seen as nodular low density within the vein. This may extend into the inferior vena cava all the way up to the right atrium. Renal cell carcinomas may spread locally to perirenal fat and adjacent organs. This is seen as strand or nodules of low density. Enlargement of renal hilar, pericaval, and periaortic nodes to 15mm or more indicates lymphatic spread. Hematogenous spread to the lung, bone, liver, adrenals, and the opposite kidney may occur. Distant metastases occasionally disappear with the removal of the primary tumor. Late appearance of metastases as long as 20 years following "cure" is also seen.
- Author
- Peter Anderson
- Posted on
- Thursday 1 August 2013
- Tags
- adrenal hemorrhage, kidney, radiology
- Albums
- Visits
- 2208
0 comments