){kind=link}
){kind=link}

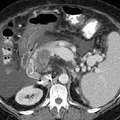
RADIOLOGY: ABDOMEN: Case# 32881: CIRRHOSIS AND PORTAL VEIN THROMBOSIS WITH THROMBOSED PORTOCAVAL SHUNT. This is a 66 year old white female with new onset of ascites and diarrhea. The liver is cirrhotic in configuration. There is splenomegaly with splenic varices and a large amount of ascites. Additionally, there is bowel wall thickening, most notably within the right colon. A side to side portocaval shunt is present which contains thrombus that extends into the confluence of the splenic vein and superior mesenteric vein. Additional thrombus extends inferiorly within the mesenteric portion of the SMV. The portal vein is not well delineated at the level of the liver hilum and the possibility of cavernous transformation is suggested. There is bilateral renal atrophy. No free air or lymphadenopathy is present. Portal vein thrombosis may be caused by hypercoagulable states, trauma, malignancy, cirrhosis, and infection. It may be accompanied by portal hypertension and its manifestations such as formation of collaterals, splenomegaly, and ascites. Portal vein thrombosis is readily diagnosed by CT and is best visualized with the incremental dynamic imaging technique. Acutely, the involved vessel enlarges, and the vessel wall may appear thickened and enhanced. There may be a small amount of contrast passing around the thrombus. The vessel itself has a relatively low central density. Serial examinations may show a change in the location or extent of thrombus, recanalization of the vessel, or retraction of the thrombus with collateral vein enlargement. Evidence of cavernous transformation of the portal vein may be seen.

- Author
- Peter Anderson
- Posted on
- Thursday 1 August 2013
- Albums
- Visits
- 1145
0 comments