){kind=link}
){kind=link}
 cirrhosis is the most frequently occurring form of the disorder. Clinical manifestations of the disease include jaundice, hypoalbuminemia, coagulation factor deficiencies, hyperstrinism, and intrahepatic scarring with increased portal venous pressure. The increase in portal venous pressure can lead to esophageal varices, rectal hemorrhiods, periumbilical venous collaterals (caput medusae), and splenomegaly. Morphologically, the liver may be enlarged or small and shrunken depending upon the progression of the disease. The nodular pattern is most often micronodular in alcoholic cirrhosis. Hepatic architecture is obscured by fibrous bands surrounding nodules of distorted liver cell plates. The fibrous bands contain proliferating bile ducts and inflammatory cells. In the final stages of cirrhosis the nodules become larger and more irregular resulting in a scarred, shrunken liver referred to as a \"hobnail liver\". Patients with cirrhosis of the liver often present with the following radiological findings. Fatty infiltration with hepatomegaly can be seen in the early stages of cirrhosis. Other characteristic findings include non-uniform attenuation due to chronic fatty infiltration and irregular fibrosis, irregular lobulated hepatic contour due to areas of atrophy and nodular regeneration, intrahepatic regenerating nodules, atrophy of the right lobe and hypertrophy of the left and caudate lobes, decreased liver volume accompanying chronic cirrhosis, increased size and prominence of the intrahepatic fissure due to shrunken liver parenchyma, signs of portal hypertension, and ascites. A ratio comparing the sizes of the caudate lobe and right lobe is a good diagnostic indicator of patients with cirrhosis. The caudate is measured transversely from the medial aspect of the caudate to the lateral aspect of the main portal vein. The right lobe is measured from this same point at the portal vein to the right lateral margin of the liver. A caudate-to-right-lobe ratio greater than 0.65 provides 96% confidence in the diagnosis of cirrhosis. A caudate-to-right-lobe ratio less then 0.6 makes cirrhosis unlikely, whereas a ratio of 0.37 is the average for normal livers.")
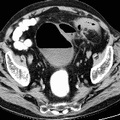
RADIOLOGY: HEPATOBILIARY: Case# 32873: CIRRHOSIS, LARGE COLLATERAL VESSELS. The patient is a 59 year old black male with alcoholic cirrhosis and known hepatocellular carcinoma. The study is compared with prior CT exam. The liver again has a cirrhotic configuration and there is now an 8 x 12 cm heterogeneous mass present in the medial segment of the left hepatic lobe. A smaller, 2 x 3 cm, hypodense lesion is also noted to be present in the posterior aspect of the lateral segment of the left hepatic lobe. Portal vein occlusion is present with cavernous transformation. Splenomegaly is again noted with a large number of splenorenal, splenogastric and esophageal varices. The enlarged spleen and varices displace the left kidney as on previous exam. The gallbladder wall is edematous without evidence of pericholecystic fluid. Liver cirrhosis is characterized by a generalized disorganization of hepatic archictecture with scarring and nodule formation. Other sequelae include liver cell damage, regenerative activity, and generalized fibrosis resulting in a nodular pattern. There is an increased incidence of hepatocelluar carcinoma associated with cirrhosis of the liver. Causes of cirrhosis include prolonged alcohol intake, viral hepatitis, biliary obstruction, Wilsons disease, and heart failure with long-standing chronic passive congestion of the liver. Alcoholic (Laennecs, nutritional) cirrhosis is the most frequently occurring form of the disorder. Clinical manifestations of the disease include jaundice, hypoalbuminemia, coagulation factor deficiencies, hyperstrinism, and intrahepatic scarring with increased portal venous pressure. The increase in portal venous pressure can lead to esophageal varices, rectal hemorrhiods, periumbilical venous collaterals (caput medusae), and splenomegaly. Morphologically, the liver may be enlarged or small and shrunken depending upon the progression of the disease. The nodular pattern is most often micronodular in alcoholic cirrhosis. Hepatic architecture is obscured by fibrous bands surrounding nodules of distorted liver cell plates. The fibrous bands contain proliferating bile ducts and inflammatory cells. In the final stages of cirrhosis the nodules become larger and more irregular resulting in a scarred, shrunken liver referred to as a "hobnail liver". Patients with cirrhosis of the liver often present with the following radiological findings. Fatty infiltration with hepatomegaly can be seen in the early stages of cirrhosis. Other characteristic findings include non-uniform attenuation due to chronic fatty infiltration and irregular fibrosis, irregular lobulated hepatic contour due to areas of atrophy and nodular regeneration, intrahepatic regenerating nodules, atrophy of the right lobe and hypertrophy of the left and caudate lobes, decreased liver volume accompanying chronic cirrhosis, increased size and prominence of the intrahepatic fissure due to shrunken liver parenchyma, signs of portal hypertension, and ascites. A ratio comparing the sizes of the caudate lobe and right lobe is a good diagnostic indicator of patients with cirrhosis. The caudate is measured transversely from the medial aspect of the caudate to the lateral aspect of the main portal vein. The right lobe is measured from this same point at the portal vein to the right lateral margin of the liver. A caudate-to-right-lobe ratio greater than 0.65 provides 96% confidence in the diagnosis of cirrhosis. A caudate-to-right-lobe ratio less then 0.6 makes cirrhosis unlikely, whereas a ratio of 0.37 is the average for normal livers.

- Author
- Peter Anderson
- Posted on
- Thursday 1 August 2013
- Albums
- Visits
- 6027
0 comments