){kind=link}
){kind=link}
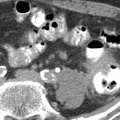
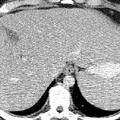
. Predisposing factors for colorectal cancer include adenomatous polyps, inherited multiple polyposis syndromes, long-standing ulcerative colitis, close relatives with colon cancer, and a low fiber, high animal fat diet. Colorectal cancer varies in gross presentation according to the region of the colon involved. Carcinoma of the rectosigmoid colon usually presents in an annular manner, often producing early bowel obstruction. Carcinoma of the right colon, however, usually does not obstruct early and frequently presents with iron deficiency anemia secondary to chronic blood loss. Colon cancer spreads by direct extension due to penetration of the colon wall, lymphatic drainage to regional nodes, through the portal system to the liver, and intraperitoneal seeding. Although barium enemas and colonoscopy are the primary methods used to initially diagnose colorectal cancer, CT is an excellent procedure for the detection of recurrence. CT findings of colon cancer include focal lobulated soft tissue mass in the colon, localized thickening of greater than 5 mm of the bowel wall, irregular lumen surface, extension of linear soft tissue densities or discrete mass into pericolic fat or adjacent organs, regional adenopathy, and liver metastases. Soft tissue masses visualized within the peritoneal cavity may signify metastases or recurrence of the cancer. Calcification in the primary tumor can be seen with mucinous adenocarcinoma.")
RADIOLOGY: GASTROINTESTINAL: GI: Case# 32856: COLON CANCER WITH APPLE-CORE LESION IN THE SIGMOID COLON. This is a 68 year old male status post laparotomy in four months ago for colon cancer. A prior abdominal CT done three months ago showed multiple liver metastases with a colonic mass at the junction of the sigmoid and descending colon. Patient is currently undergoing 5-FU chemotherapy and this study has been ordered for re-evaluation. There is a marked decrease in size of the multiple hepatic metastases that were previously identified. As an index lesion, a low attenuation mass in the anterior segment of the right lobe which previously measured 2 cm today measures 6 mm. A 1.5 x .8 cm peripancreatic node is seen. The kidneys and small bowel reveal no abnormalities. Distention of the distal colon with rectal contrast showed an apple core mass at the junction of the sigmoid and descending colon. At the site of the neoplasm, the colon abuts the left psoas muscle and the border between psoas and colon is not well defined. Colorectal adenocarcinoma is one of the most common neoplasms encountered in the affluent countries of the Western world. The disease exhibits a peak age incidence in the sixth and seventh decades. It is associated with increased serum concentration of carcinoembryonic antigen (CEA). Predisposing factors for colorectal cancer include adenomatous polyps, inherited multiple polyposis syndromes, long-standing ulcerative colitis, close relatives with colon cancer, and a low fiber, high animal fat diet. Colorectal cancer varies in gross presentation according to the region of the colon involved. Carcinoma of the rectosigmoid colon usually presents in an annular manner, often producing early bowel obstruction. Carcinoma of the right colon, however, usually does not obstruct early and frequently presents with iron deficiency anemia secondary to chronic blood loss. Colon cancer spreads by direct extension due to penetration of the colon wall, lymphatic drainage to regional nodes, through the portal system to the liver, and intraperitoneal seeding. Although barium enemas and colonoscopy are the primary methods used to initially diagnose colorectal cancer, CT is an excellent procedure for the detection of recurrence. CT findings of colon cancer include focal lobulated soft tissue mass in the colon, localized thickening of greater than 5 mm of the bowel wall, irregular lumen surface, extension of linear soft tissue densities or discrete mass into pericolic fat or adjacent organs, regional adenopathy, and liver metastases. Soft tissue masses visualized within the peritoneal cavity may signify metastases or recurrence of the cancer. Calcification in the primary tumor can be seen with mucinous adenocarcinoma.
- Author
- Peter Anderson
- Posted on
- Thursday 1 August 2013
- Tags
- gastrointestinal, radiology
- Albums
- Visits
- 1055
0 comments