){kind=link}
){kind=link}

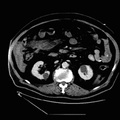
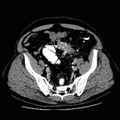
RADIOLOGY: HEPATOBILIARY: Case# 32776: HEPATIC ABSCESSES AND INFARCTS, S/P OLTX. The patient is a 54-year-old male, s/p orthotopic liver transplant six months ago, with elevated LFTs and multiple hypo- and hyperechogenic areas on ultrasound. RIs on ultrasound are less than .5, worrisome for hepatic artery stenosis/occlusion of both left and right hepatic arteries. There are multiple low attenuation regions seen scattered throughout all segments of the liver. There are three large wedge-shaped areas, the largest in the posterior segment of the right lobe, next lateral segment of the left lobe, and the third straddling the anteroposterior lobe of the liver. These regions all have bubbles of air or air fluid levels within. The largest collection appears to be in the right posterior segment. The portal vein appears unremarkable. No enhancing masses noted. There is no biliary ductal dilatation. There is a nonspecific portocaval node. The spleen is enlarged. Pyogenic liver abscesses occur predominantly in individuals with other underlying disorders, most commonly biliary tract disease. Abscesses may also occur following hepatic transplantation. Clinical findings are nonspecific with fever and jaundice being the most common. Diagnosis is best made by contrast-enhanced CT or ultrasound. Pyogenic abscesses are usually solitary and often multiloculated with thickened enhancing walls. Gas is present in about 20% of cases. Amoebic abscesses are also solitary lesions. Pyogenic abscesses may be distinguished from amoebic abscesses on the basis of clinical findings. Whereas patients with pyogenic abscesses are usually septic, patients with amoebic abscesses are not, and they usually have a history of travel to an endemic area. Pyogenic abscesses require drainage while amoebic abscesses do not and may be treated with antibiotics. Hepatic infarcts may also occur following hepatic transplantation. Partial or complete hepatic artery obstruction may present as lobar areas of inhomogeneous low attenuation and may require retransplantation. Occlusion of hepatic arterial branches may produce round or oval central lesions or wedge-shaped peripheral lesions that may contain gas, giving the appearance of an abscess. These infarcts may be seen as poorly demarcated areas that progress to become more confluent and delineated.
- Author
- Peter Anderson
- Posted on
- Thursday 1 August 2013
- Tags
- hepatobiliary, radiology
- Albums
- Visits
- 877
0 comments