){kind=link}
){kind=link}
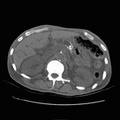
 which was complicated by pancreatitis with ductal disruption and pseudocyst formation. The patient subsequently underwent cystogastrostomy. She now presents with abdominal pain. A 6 x 7 cm pancreatic pseudocyst extends anteriorly from the pancreatic neck and is in contacwith the posterior portion of the gastric antrum. The head of the pancreas is somewhat prominent. The tail of the pancreas is attenuated. The splenic vein is prominent suggesting mild compression of the portal vein by the pseudocyst. Pancreatic pseudocysts are usually the sequelae of pancreatitis, most often associated with the subacute or chronic varieties. Peripancreatic fluid collections in the setting of acute pancreatitis are not pseduocysts. A pseudocyst is a cystic structure with a thick, fibrous wall and is not lined with epithelium (hence, it is not a true cyst). A pseudocyst may have a persistent connection to the pancreatic duct which may be demonstrated by ERCP. Typically, an uncomplicated pseudocyst will have a homogeneous water density. Increased density or inhomogeneity indicate some complicating factor such as hemorrhage or infection. Psuedocysts may also form in the walls of bowel (stomach, duodenum, colon) due to extension of pancreatic enzymes into the surrounding tissues.")
RADIOLOGY: PANCREAS: Case# 72: PANCREATIC PSEUDOCYST. 46-year-old white female S/P ERCP (14 months prior to scan) which was complicated by pancreatitis with ductal disruption and pseudocyst formation. The patient subsequently underwent cystogastrostomy. She now presents with abdominal pain. A 6 x 7 cm pancreatic pseudocyst extends anteriorly from the pancreatic neck and is in contacwith the posterior portion of the gastric antrum. The head of the pancreas is somewhat prominent. The tail of the pancreas is attenuated. The splenic vein is prominent suggesting mild compression of the portal vein by the pseudocyst. Pancreatic pseudocysts are usually the sequelae of pancreatitis, most often associated with the subacute or chronic varieties. Peripancreatic fluid collections in the setting of acute pancreatitis are not pseduocysts. A pseudocyst is a cystic structure with a thick, fibrous wall and is not lined with epithelium (hence, it is not a true cyst). A pseudocyst may have a persistent connection to the pancreatic duct which may be demonstrated by ERCP. Typically, an uncomplicated pseudocyst will have a homogeneous water density. Increased density or inhomogeneity indicate some complicating factor such as hemorrhage or infection. Psuedocysts may also form in the walls of bowel (stomach, duodenum, colon) due to extension of pancreatic enzymes into the surrounding tissues.

- Author
- Peter Anderson
- Posted on
- Thursday 1 August 2013
- Albums
- Visits
- 1613
0 comments