){kind=link}
){kind=link}

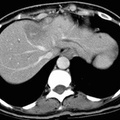
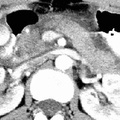
RADIOLOGY: PANCREAS: Case# 50: PANCREATIC ADENOCARCINOMA. The patient is a 55 year old black female with a pancreatic head mass seen on ultrasound. A 3.0 x 4.0 cm heterogeneously enhancing mass is seen at the region of the pancreatic neck. This mass compresses the common bile duct and is associated with a large amount of intrahepatic and extrahepatic biliary ductal dilatation, as well as dilatation of the pancreatic duct within the tail. This pancreatic mass also compresses the portal vein, splenic vein, inferior vena cava, and the superior mesenteric vein; however, each of these veins is patent. The pancreatic mass also abuts and possibly invades the posterior gastric antral wall. Multiple enlarged peripancreatic, periaortic, porta hepatic, portocaval, and gastric ligament lymph nodes are identified. A focal area of low attenuation is seen within the medial aspect of the left hepatic lobe which most likely represents focal fatty infiltration; however, metastasis cannot be entirely excluded. This almost uniformly fatal cancer is the 4th most common malignant tumor accounting for 5% of cancer deaths in the United States. Symptoms are usually nonspecific and insidious such that the cancer is advanced by the time of diagnosis. Most cancers occur in the head of the pancreas and are usually adenocarcinomas arising from ductal cells. The sensitivity of CT scan in diagnosing pancreatic carcinoma is approximately 95% whereas that of ultrasound is less than 80% for cancer of the head and 40% for the tail. The primary finding on CT is a focal mass;however, if no mass is present, other findings may suggest neoplasm. First, the pancreas may become more heterogeneous in density with age. Thus, a focal region of homogeneous soft tissue density might raise suspicion of a carcinoma. The presence of both a dilated common bile duct and a dilated main pancreatic duct in the absence of calculus suggests ampullary or pancreatic head neoplasm, but this may also be seen in benign disease. The finding of a dilated main pancreatic duct in the body or tail but not in the head or neck suggests neoplasm, and finally, the finding of rounded convex borders of both anterior and posterior surfaces of the uncinate process raises suspicion for carcinoma. Ten to fifteen percent of patients will have potentially resectable tumors, and they may be distinguished by CT findings. Signs of potential resectability include an isolated pancreatic mass with or without dilatation of the bile and pancreatic ducts and combined bile-pancreatic duct dilatation without an identifiable pancreatic mass. Extension of the tumor beyond the margins of the pancreas, involvement of adjacent organs or the SMA, liver metastases, ascites, and regional adenopathy are signs of unresectability. Unfortunately, most of those who undergo resection eventually die of pancreatic cancer.
- Author
- Peter Anderson
- Posted on
- Thursday 1 August 2013
- Albums
- Visits
- 1696
0 comments