){kind=link}
){kind=link}

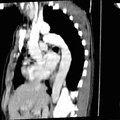
RADIOLOGY: AORTA: Case# 31: LEAKING AAA/DISSECTION. 56 year old female with a six day history of abdominal and back pain gradually increasing in severity. Irregularity of the right and anterior walls of the descending aorta begins at about the level of the diaphragmatic crus. The aorta is dilated and contains a large amount of thrombus. The thrombus has a crescentic shape while the opacified lumen has a lenticular configuration. The above findings are consistent with aortic dissection with a thrombosed false channel. A small amount of contrast extravasates into the periaortic soft tissues at the cephalad extent of the dissection. Abdominal aortic aneurysms usually occur in the setting of atherosclerotic disease but may be caused by syphilis, by extension of a dissection from above, or by connective tissue disorders such as Takayasus arteritis. Complications of abdominal aortic aneurysm include rupture, peripheral embolization, thrombosis, and infection. The incidence of rupture increases with increasing aneurysm size above 4 cm. Rupture usually occurs into the left retroperitoneal space and rarely into the gastrointestinal tract and inferior vena cava. If a ruptured or leaking aneurysm is suspected, CT should be done with contrast enhancement. Typical findings include obscuration or anterior displacement of the aneurysm by an irregular high density mass or collection that extends into one or both perirenal spaces. The wall of the aneurysm may be identified by calcifications while the lumen enhances. Other findings include anterior displacement of the kidney by hematoma, enlargement or obscuration of the psoas muscle, and a focally indistinct aortic margin that corresponds to the site of rupture. In contrast, a chronic pseudoaneurysm appears as a well-defined, ususally round mass with attenuation similar or lower than that of the native aorta on noncontrasted images.

- Author
- Peter Anderson
- Posted on
- Thursday 1 August 2013
- Albums
- Visits
- 1834
0 comments