){kind=link}
){kind=link}
 the aortic arch; (2) the proximal aortic root and descending aorta near the level of the pulmonary artery; (3) the more distal descending thoracic aorta. Newer helical CT scanners allow rapid scanning of the arch during bolus contrast injection eliminating the need for the \"three level scan\". Two passes can be made throught the aortic arch early in the contrast injection. In a patient with dissection, the intimal flap may be delineated by contrast filling both the true and false channels. One of the channels may fill slowly, thus requiring the use of images late in the sequence to make the diagnosis. A false channel that contains a clot may not opacify and in such a case, may be difficult to distinguish from a clot-filled atherosclerotic aneurysm. Dissections, however, are usually longer than clot-filled aneurysms and may produce an abrupt change in aortic caliber and thickening of the aortic wall. Streak artifacts due to wall motion or vascular pulsations may mimic an intimal flap. Streak artifacts are usually seen in the descending aorta adjacent to the left heart. They are usually less well-defined than a true intimal flap, extending beyond the edge of the aorta and inconsistently seen from level to level. Repeat CT should be done in cases of uncertainty.")
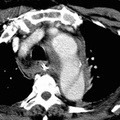
RADIOLOGY: AORTA: Case# 23: TYPE 3 OR TYPE B AORTIC DISSECTION. 68-year-old white male with sudden onset chest pain. There is aortic dissection of the descending thoracic and abdominal aorta starting near the origin of left subclavian artery and extending down to the level of aortobifem bypass graft. No intimal flap is noted in the ascending aorta. There is minimal irregularity of the thoracic aortic wall near the left subclavian region along with para-aortic hematoma which has CT attenuation value of 45-50 HU. The celiac, SMA, and right renal artery appear to arise from the true lumen whereas the left renal artery appears to arise from the false lumen. CT has to a large degree replaced arteriography in diagnosing aortic dissection and determining its type and location. The diagnosis is made by the demonstration of an intimal flap, displaced inward from the edge of the aorta and lying between the true and false channels. In Dailys classification, types A and B are described with type A being more common. Type A involves the ascending aorta and is usually treated surgically because of the potential for retrograde dissection. Type B involves the area distal to the left subclavian artery and is treated medically. CT is used for screening those with suspected aortic dissection and for follow-up of patients previously diagnosed with dissection. It should be performed with bolus contrast enhancement and dynamic scanning at three levels: (1) the aortic arch; (2) the proximal aortic root and descending aorta near the level of the pulmonary artery; (3) the more distal descending thoracic aorta. Newer helical CT scanners allow rapid scanning of the arch during bolus contrast injection eliminating the need for the "three level scan". Two passes can be made throught the aortic arch early in the contrast injection. In a patient with dissection, the intimal flap may be delineated by contrast filling both the true and false channels. One of the channels may fill slowly, thus requiring the use of images late in the sequence to make the diagnosis. A false channel that contains a clot may not opacify and in such a case, may be difficult to distinguish from a clot-filled atherosclerotic aneurysm. Dissections, however, are usually longer than clot-filled aneurysms and may produce an abrupt change in aortic caliber and thickening of the aortic wall. Streak artifacts due to wall motion or vascular pulsations may mimic an intimal flap. Streak artifacts are usually seen in the descending aorta adjacent to the left heart. They are usually less well-defined than a true intimal flap, extending beyond the edge of the aorta and inconsistently seen from level to level. Repeat CT should be done in cases of uncertainty.

- Author
- Peter Anderson
- Posted on
- Thursday 1 August 2013
- Albums
- Visits
- 1852
0 comments