Difference between revisions of "IPLab:Lab 3:Acute Appendicitis"
Seung Park (talk | contribs) |
(→Images) |
||
| (4 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| − | + | An 11-year-old male was admitted to the hospital with a complaint of 8 hours of severe pain in the right lower quadrant of the abdomen accompanied by nausea, vomiting, and diarrhea. On admission his temperature was 101° F and he had a leukocytosis of 21,200 cells/cmm with a shift to the left. An exploratory laparotomy revealed an inflamed appendix, retrocecal in location, which was adherent to the wall of the colon. | |
| − | + | The serosal surface of the appendix was covered with friable granular material. The lumen was dilated and contained a purulent exudate as well as a fecalith. The wall measured up to 0.4 cm in thickness. | |
| − | The serosal surface of the appendix was covered with friable granular material. The lumen was dilated and contained a purulent exudate as well as a fecalith. The wall measured up to 0.4 cm in thickness. | ||
== Images == | == Images == | ||
<gallery heights="250px" widths="250px"> | <gallery heights="250px" widths="250px"> | ||
File:IPLab3AcuteAppendicitis1.jpg|This is a gross photograph of the appendix which was removed from this patient with acute appendicitis. Note the rough, shaggy material (arrows) on the surface due to deposition of fibrin and inflammatory cells. | File:IPLab3AcuteAppendicitis1.jpg|This is a gross photograph of the appendix which was removed from this patient with acute appendicitis. Note the rough, shaggy material (arrows) on the surface due to deposition of fibrin and inflammatory cells. | ||
| − | File: | + | File:IPLab3AcuteAppendicitis2b.jpg|This is a low-power photomicrograph of a normal appendix on the right and this appendix with an acute inflammatory response on the left. Note the focal areas of blue-stained lymphoid tissue which is normal for the normal appendix. Compare this with the increased size of the inflamed appendix (left) due to inflammatory cells and edema. |
| − | File: | + | File:IPLab3AcuteAppendicitis2x.jpg|Photomicrograph of this appendix with acute inflammatory response. Note the extensive distribution of cells throughout the wall of this appendix with acute appendicitis. The blue color is due to the presence of many inflammatory cells, although at this low power these individual cells cannot be specifically identified. |
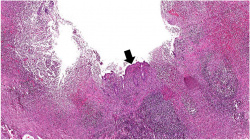
| − | + | File:IPLab3AcuteAppendicitis3b.jpg|This is a photomicrograph showing the serosal surface of the appendix with the layer of fibrinopurulent exudate noted in the gross photo (1). The muscularis (M) and the submucosa (S) also have a robust inflammatory cell infiltrate. | |
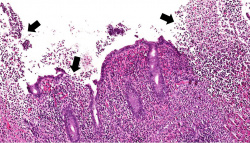
| − | File: | + | File:IPLab3AcuteAppendicitis4b.jpg|This photomicrograph of the lumen shows the mucosal surface with a small area of normal mucosal epithelium (arrow). This area is surrounded by the ulcerated mucosa with inflammatory infiltrates comprising primarily neutrophils with a few lymphocytes and macrophages. |
| − | File: | + | File:IPLab3AcuteAppendicitis5b.jpg|TThis higher-power photomicrograph of the mucosal surface shows the loss of normal mucosal epithelium (arrows) and the inflammatory infiltrate. The principal inflammatory cell in this case of acute appendicitis is the neutrophil. |
File:IPLab3AcuteAppendicitis7.jpg|This is a gross photograph of the open abdominal cavity of a patient with acute appendicitis. In this patient, there had been rupture of the appendix with spillage of intestinal contents into the abdominal cavity. This spillage resulted in an acute abdomen with widespread inflammation throughout the abdominal cavity. Note the roughened surface of the mesenteric tissue (arrow) due to deposition of fibrin over much of the surface. | File:IPLab3AcuteAppendicitis7.jpg|This is a gross photograph of the open abdominal cavity of a patient with acute appendicitis. In this patient, there had been rupture of the appendix with spillage of intestinal contents into the abdominal cavity. This spillage resulted in an acute abdomen with widespread inflammation throughout the abdominal cavity. Note the roughened surface of the mesenteric tissue (arrow) due to deposition of fibrin over much of the surface. | ||
File:IPLab3AcuteAppendicitis8.jpg|This is a gross photograph of another example of peritonitis. Again note the fibrinosuppurative exudate covering the abdominal organs (arrows). | File:IPLab3AcuteAppendicitis8.jpg|This is a gross photograph of another example of peritonitis. Again note the fibrinosuppurative exudate covering the abdominal organs (arrows). | ||
| Line 18: | Line 17: | ||
== Virtual Microscopy == | == Virtual Microscopy == | ||
| + | ===Appendicitis (left) and Normal Appendix (right) === | ||
<peir-vm>IPLab3AcuteAppendicitis</peir-vm> | <peir-vm>IPLab3AcuteAppendicitis</peir-vm> | ||
Latest revision as of 22:59, 19 June 2020
Contents
Clinical Summary[edit]
An 11-year-old male was admitted to the hospital with a complaint of 8 hours of severe pain in the right lower quadrant of the abdomen accompanied by nausea, vomiting, and diarrhea. On admission his temperature was 101° F and he had a leukocytosis of 21,200 cells/cmm with a shift to the left. An exploratory laparotomy revealed an inflamed appendix, retrocecal in location, which was adherent to the wall of the colon.
The serosal surface of the appendix was covered with friable granular material. The lumen was dilated and contained a purulent exudate as well as a fecalith. The wall measured up to 0.4 cm in thickness.
Images[edit]

This is a gross photograph of the appendix which was removed from this patient with acute appendicitis. Note the rough, shaggy material (arrows) on the surface due to deposition of fibrin and inflammatory cells.
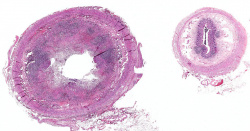
This is a low-power photomicrograph of a normal appendix on the right and this appendix with an acute inflammatory response on the left. Note the focal areas of blue-stained lymphoid tissue which is normal for the normal appendix. Compare this with the increased size of the inflamed appendix (left) due to inflammatory cells and edema.

Photomicrograph of this appendix with acute inflammatory response. Note the extensive distribution of cells throughout the wall of this appendix with acute appendicitis. The blue color is due to the presence of many inflammatory cells, although at this low power these individual cells cannot be specifically identified.

This is a photomicrograph showing the serosal surface of the appendix with the layer of fibrinopurulent exudate noted in the gross photo (1). The muscularis (M) and the submucosa (S) also have a robust inflammatory cell infiltrate.
This photomicrograph of the lumen shows the mucosal surface with a small area of normal mucosal epithelium (arrow). This area is surrounded by the ulcerated mucosa with inflammatory infiltrates comprising primarily neutrophils with a few lymphocytes and macrophages.
TThis higher-power photomicrograph of the mucosal surface shows the loss of normal mucosal epithelium (arrows) and the inflammatory infiltrate. The principal inflammatory cell in this case of acute appendicitis is the neutrophil.

This is a gross photograph of the open abdominal cavity of a patient with acute appendicitis. In this patient, there had been rupture of the appendix with spillage of intestinal contents into the abdominal cavity. This spillage resulted in an acute abdomen with widespread inflammation throughout the abdominal cavity. Note the roughened surface of the mesenteric tissue (arrow) due to deposition of fibrin over much of the surface.

This is a gross photograph of another example of peritonitis. Again note the fibrinosuppurative exudate covering the abdominal organs (arrows).








Virtual Microscopy[edit]
Appendicitis (left) and Normal Appendix (right)[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Appendicitis
- Merck Manual: Introduction to Acute Abdomen and Surgical Gastroenterology
- Merck Manual: Appendicitis
Journal Articles[edit]
- Helmer KS, Robinson EK, Lally KP, Vasquez JC, Kwong KL, Liu TH, Mercer DW. Standardized patient care guidelines reduce infectious morbidity in appendectomy patients. Am J Surg 2002 Jun;183(6):608-13.
Images[edit]
A shift to the left indicates an increased ratio of immature PMNs (bands) to mature PMNs (segs).
Friable material is easily crumbled.
A fecalith is a hardened collection of fecal matter formed within the intestine.
An infiltrate is an accumulation of cells in the lung parenchyma--this is a sign of pneumonia.
An infiltrate is an accumulation of cells in the lung parenchyma--this is a sign of pneumonia.