IPLab:Lab 12:Thoracic Mesothelioma
Contents
Clinical Summary[edit]
This 61-year-old white male had a known history of asbestos exposure as well as a 40 pack-year history of smoking and coronary artery disease. Two years ago an open lung biopsy showed a thoracic mesothelioma. At this admission the patient complained of shortness of breath, orthopnea, and pedal edema. Physical examination revealed mild respiratory distress on nasal oxygen and a dull left hemothorax. Chest x-ray demonstrated a left hemothorax opacity, small right pleural effusions, and pleural plaques. The patient subsequently developed atrial fibrillation and immediately prior to his death he suffered a stroke.
At autopsy tumor plaque covered 100% of the left lung, 50% of the right lung, and extended into the thoracic wall, the diaphragm, and the heart.
Images[edit]
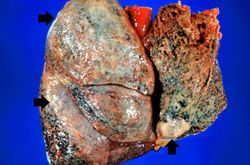
This is a gross photograph of the lungs removed at autopsy. There is thickening of the pleural surface due to the tumor (arrows). The apical portion of the left lobe of the lung was ripped while trying to sever the adhesions between the lung and the chest wall.
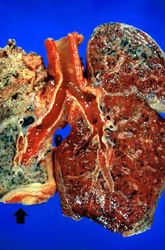
This is a gross photograph of cut sections of the lungs. The right lung is congested. The left lung is shrunken and filled with tumor. There is a thick layer of tumor along the inferior portion of the lung (arrow).
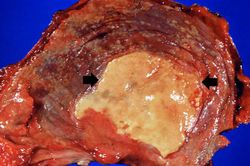
This is a gross photograph of the thoracic surface of the diaphragm demonstrating the distinctive fibrocalcific plaque (arrows) produced by mesothelioma and multiple smaller plaques over the pleural surface of the diaphragm.
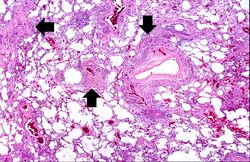
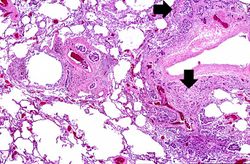
This is a low-power photomicrograph of a section of the left lung. At this magnification you can see areas of consolidation (arrows), especially around blood vessels.
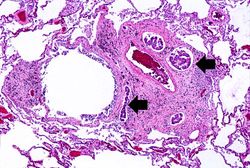
This higher-power photomicrograph of left lung shows areas of consolidation and fibrosis (arrows). Also note that in many of these areas there are clusters of blue cells.
In this higher-power photomicrograph the clusters of tumor cells (arrows) can be appreciated.
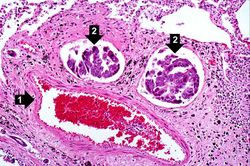
In this higher-power photomicrograph there is a blood vessel (1) and adjacent lymphatics that contain tumor cells (2). There are also accumulations of brown material adjacent to these vessels.
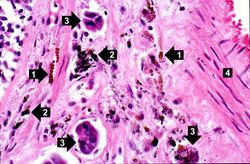
This high-power photomicrograph shows brown asbestos bodies (1), accumulations of anthracotic pigment (2), and tumor cells (3) all adjacent to a blood vessel (4).
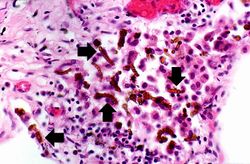
This is a high-power photomicrograph of the brown asbestos bodies showing the characteristic beaded appearance (arrows).
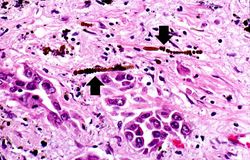
Another high-power photomicrograph of the brown asbestos bodies showing the characteristic beaded appearance (arrows). Tumor cells are evident adjacent to the asbestos bodies.
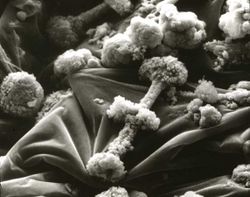
Scanning electron micrograph of asbestos bodies. Note the rough surface and the beaded appearance caused by the material adhering to the surface of the asbestos fiber.











Virtual Microscopy[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Malignant Mesothelioma Imaging
- eMedicine Medical Library: Asbestosis Imaging
- Merck Manual: Asbestos-Related Disorders
Journal Articles[edit]
- Whitaker D. The cytology of malignant mesothelioma. Cytopathology 2000 Jun;11(3):139-51.
- Johnson JS, Edwards JM. Malignant mesothelioma mimicking squamous carcinoma in a pleural fluid aspirate. Cytopathology 2001 Feb;12(1):54-6.
Images[edit]
| |||||
A pack-year denotes smoking one pack of cigarettes per day for one year.
Shortness of breath is a common clinical manifestation of heart failure.
Pleural effusion is the presence of fluid in the pleural space. Increased hydrostatic pressure in the pulmonary vasculature, as seen in heart failure, is one cause of pleural effusion.
Anthracotic pigment is coal dust deposited in the lungs--it is seen in coal miners, city-dwellers, and smokers.
A normal PaCO2 is 35 to 45 mmHg.