IPLab:Lab 12:COPD
Contents
Clinical SummaryEdit
This 64-year-old man was hospitalized because of increasing shortness of breath, cough, increasing sputum production, and fever. The patient had a 75 pack-year history of cigarette smoking. On admission his respiratory rate was 20 breaths per minute and his pulse was 110 bpm. On room air his PaO2 was 46 mm Hg, his PaCO2 was 62 mm Hg , and the pH was 7.26. Chest x-ray showed a low, flattened diaphragm, and markedly lucent regions in the upper lung fields suggesting areas of emphysema. Despite appropriate therapy he suffered acute respiratory failure and could not be resuscitated.
Pertinent autopsy findings included emphysema with moderate mucous plugging of bronchi. Right ventricular hypertrophy and dilation were also noted.
Autopsy FindingsEdit
Pertinent autopsy findings included emphysema with moderate mucous plugging of bronchi. Right ventricular hypertrophy and dilation were also noted.
ImagesEdit
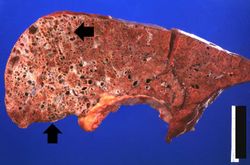
This gross photograph of lung taken at autopsy demonstrates the degree of emphysematous change (arrows). Also note that the rest of the lung is consolidated, indicating a pneumonia.
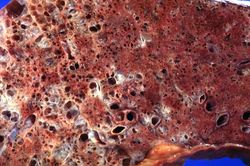
This is a higher-power view of the lung showing the emphysematous change.
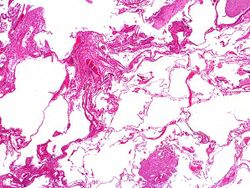
This low-power photomicrograph of the lung demonstrates the enlarged air spaces indicative of emphysematous change.
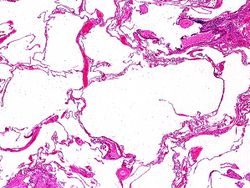
This higher-power photomicrograph of the lung shows more clearly the enlarged air spaces indicative of emphysematous change.

This gross photograph of the heart taken at autopsy demonstrates right ventricular hypertrophy and dilatation (arrows).





Study QuestionsEdit
Additional ResourcesEdit
ReferenceEdit
- eMedicine Medical Library: Chronic Obstructive Pulmonary Disease and Emphysema in Emergency Medicine
- eMedicine Medical Library: Chronic Obstructive Pulmonary Disease
- eMedicine Medical Library: Nicotine Addiction
- Merck Manual: Chronic Obstructive Pulmonary Disease
Journal ArticlesEdit
- Franks TJ, Galvin JR. Smoking-Related Interstitial Lung Disease. Arch Pathol Lab Med. 2015;139:974–977.
ImagesEdit
Related IPLab CasesEdit
Shortness of breath is a common clinical manifestation of heart failure.
A pack-year denotes smoking one pack of cigarettes per day for one year.
A normal respiratory rate is 10 to 20 breaths per minute.
A normal pulse rate is 60 to 100 bpm.
A normal PaO2 is 80 to 105 mm Hg.
A normal PaCO2 is 35 to 45 mmHg.
A normal arterial pH is 7.35 to 7.45.
Pulmonary emphysema is a condition in which the air spaces distal to the terminal bronchioles are permanently increased in size due to either destruction of the wall or alveolar dilatation.
Consolidation is the filling of lung air spaces with exudate--this is a sign of pneumonia.
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.