Difference between revisions of "Cytologically Yours: CoW: 20131202"
(→Resident Questions) |
|||
| (16 intermediate revisions by the same user not shown) | |||
| Line 20: | Line 20: | ||
* CT of abdomen and pelvis showed adenopathy adjacent to the aorta and inferior to the vena cava at the level of the right kidney. The largest node measured 4 cm in greatest dimension. | * CT of abdomen and pelvis showed adenopathy adjacent to the aorta and inferior to the vena cava at the level of the right kidney. The largest node measured 4 cm in greatest dimension. | ||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
==Pathology== | ==Pathology== | ||
| Line 36: | Line 30: | ||
</gallery> | </gallery> | ||
| + | |||
====Resident Questions==== | ====Resident Questions==== | ||
* <spoiler text="What is your differential diagnosis?">These groups of cells demonstrate malignant appearing cells in a background of an otherwise benign appearing lymphoid background. The atypical cells are scattered, with large nucleoli and several binucleate forms. In addition, there seem to be an increased number of eosinophils in the background. The differential diagnosis includes Hodgkin lymphoma; however, the possibility of the large atypical cells being melanoma cannot be ruled out. </spoiler> | * <spoiler text="What is your differential diagnosis?">These groups of cells demonstrate malignant appearing cells in a background of an otherwise benign appearing lymphoid background. The atypical cells are scattered, with large nucleoli and several binucleate forms. In addition, there seem to be an increased number of eosinophils in the background. The differential diagnosis includes Hodgkin lymphoma; however, the possibility of the large atypical cells being melanoma cannot be ruled out. </spoiler> | ||
* <spoiler text="What ancillary tests would you recommend?">For this patient, we recommended that the radiologist perform a biopsy of the lesion so that it could be sent for immunohistochemical workup. Since the overall percentage of the atypical cells were low, we were worried that a cell block would not contain enough of the malignant cells for additional stains. We also sent the lymph node for flow since a hematologic malignancy was suspected; however, with Hodgkin lymphoma, we don't expect any diagnostic findings from flow cytometry.</spoiler> | * <spoiler text="What ancillary tests would you recommend?">For this patient, we recommended that the radiologist perform a biopsy of the lesion so that it could be sent for immunohistochemical workup. Since the overall percentage of the atypical cells were low, we were worried that a cell block would not contain enough of the malignant cells for additional stains. We also sent the lymph node for flow since a hematologic malignancy was suspected; however, with Hodgkin lymphoma, we don't expect any diagnostic findings from flow cytometry.</spoiler> | ||
| + | * <spoiler text="What immunohistochemical stains would you do?">CD15, CD30, and PAX5 would stain tumor cells in Hodkin lymphoma. Mart1, HMB45, and S100 could be used to rule out melanoma. Other additional stain in a lymphoma versus melanoma workup might include CD3, CD20, and keratin.</spoiler> | ||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | + | <div class="usermessage mw-customtoggle-diagnosis" style="cursor:pointer">Click here to toggle the diagnosis and discussion.</div> | |
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | |||
| − | <div class="usermessage mw-customtoggle-diagnosis" style="cursor:pointer">Click here to toggle the diagnosis and | ||
<div class="mw-collapsible mw-collapsed" id="mw-customcollapsible-diagnosis"> | <div class="mw-collapsible mw-collapsed" id="mw-customcollapsible-diagnosis"> | ||
<div class="mw-collapsible-content"> | <div class="mw-collapsible-content"> | ||
| Line 68: | Line 45: | ||
===Cytology=== | ===Cytology=== | ||
* '''Positive for malignancy, the differential diagnosis includes melanoma and Hodgkin lymphoma'''. | * '''Positive for malignancy, the differential diagnosis includes melanoma and Hodgkin lymphoma'''. | ||
| + | |||
===Biopsy=== | ===Biopsy=== | ||
| + | <gallery heights="250px" widths="250px"> | ||
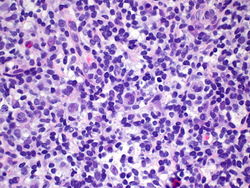
| + | CytologicallyYoursCoW20131202Biopsy1.jpg|20x magnification of lymph node core biopsy. | ||
| + | CytologicallyYoursCoW20131202Biopsy2.jpg|40x magnification of lymph node core biopsy. | ||
| + | CytologicallyYoursCoW20131202Biopsy3.jpg|CD 15 with membranous staining. | ||
| + | CytologicallyYoursCoW20131202Biopsy4.jpg|CD 30 with membranous staining. | ||
| + | |||
| + | </gallery> | ||
| + | |||
| + | ===Biopsy Diagnosis=== | ||
* '''Classical Hodgkin lymphoma, favor mixed type'''. | * '''Classical Hodgkin lymphoma, favor mixed type'''. | ||
| + | ** CD15 Positive in tumor cells | ||
| + | ** CD30 Positive in tumor cells | ||
| + | ** PAX5 Weakly positive | ||
| + | ** CD20 Positive in background lymphocytes | ||
| + | ** CD3 Positive in background lymphocytes | ||
| + | ** S100 Negative | ||
| + | ** Mart1 Negative | ||
| + | ** HMB45 Negative | ||
| + | |||
| + | ===Discussion=== | ||
| + | The features of Hodgkin lymphoma include atypical (Hodgkin cells) and Reed-Sternberg cells. The nucleus should be 3-4x the size of a small lymphocyte. In classic Hodgkin lymphoma, scattered eosinophils, plasma cells, histiocytes, and a predominately CD3+ lymphocyte population will be seen in the background. The immunophenotype of classic Hodgkin lymphoma shows CD15, CD30, MUM1, and weak PAX5 positivity. Histology is usually needed to subtype Hodgkin lymphoma. | ||
| − | |||
| − | |||
</div></div> | </div></div> | ||
Latest revision as of 21:52, 15 January 2014
Contents
Clinical Summary
The patient is an 60 year old male with a remote history of an abdominal melanoma that was excised with negative margins. The patient has been experiencing lower back pain for the past several months and has received epidural injections. As a part of the workup, the patient had a CT which revealed retroperitoneal lymphadenopathy. A CT guided fine needle aspiration and biopsy of a paracaval lymph node was performed.
Past Medical History
- 2003 Melanoma
- Diabetes
- Hypertension
Past Surgical History
- 2013 Arthroscopic knee surgery
- 2003 Excision of melanoma
- 2002 Discectomy
Clinical Plan
The differential diagnosis for otherwise asymptomatic lymphadenopathy in this patient is melanoma, lymphoma, or occult malignancy.
Radiology
- PET CT showed hypermetabolic activity with an SUV of 12.7.
- CT of abdomen and pelvis showed adenopathy adjacent to the aorta and inferior to the vena cava at the level of the right kidney. The largest node measured 4 cm in greatest dimension.
Pathology
Cytology
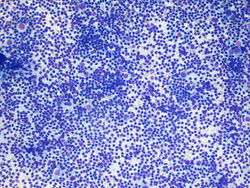
10x magnification of paracaval lymph node. There is a polymorphic lymphoid population with scattered large atypical cells.
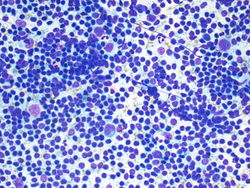
20x magnification of paracaval lymph node. There are small lymphocytes with background lymphoglandular bodies. Scattered eosinophils and large atypical cells with prominent nucleoli.
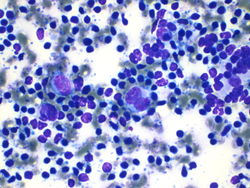
40x magnification of paracaval lymph node. There are atypical binucleated cells among the large atypical cells.



Resident Questions
Final Diagnosis
Cytology
- Positive for malignancy, the differential diagnosis includes melanoma and Hodgkin lymphoma.
Biopsy
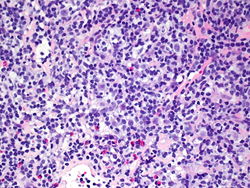
20x magnification of lymph node core biopsy.
40x magnification of lymph node core biopsy.
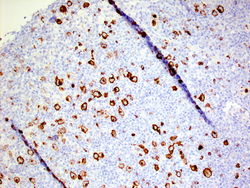
CD 15 with membranous staining.
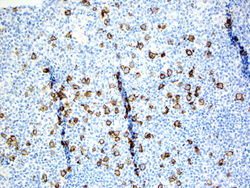
CD 30 with membranous staining.




Biopsy Diagnosis
- Classical Hodgkin lymphoma, favor mixed type.
- CD15 Positive in tumor cells
- CD30 Positive in tumor cells
- PAX5 Weakly positive
- CD20 Positive in background lymphocytes
- CD3 Positive in background lymphocytes
- S100 Negative
- Mart1 Negative
- HMB45 Negative
Discussion
The features of Hodgkin lymphoma include atypical (Hodgkin cells) and Reed-Sternberg cells. The nucleus should be 3-4x the size of a small lymphocyte. In classic Hodgkin lymphoma, scattered eosinophils, plasma cells, histiocytes, and a predominately CD3+ lymphocyte population will be seen in the background. The immunophenotype of classic Hodgkin lymphoma shows CD15, CD30, MUM1, and weak PAX5 positivity. Histology is usually needed to subtype Hodgkin lymphoma.
| ||||||||