Cytologically Yours: CoW: 20131118
Contents
Clinical History
The patient is a 49 year old male who was found to have an enlarging nodule in the right lower lobe on CT scan. The nodule was first identified in March of 2013 and a repeat CT scan in June 2013 showed it had increased in size from 1.4 cm in greatest dimension to 2.0 cm in greatest dimension. The patient denied fever, chills, and weight loss.
Past Medical History
- Coronary artery disease stats post coronary artery bypass grafting in 2008
- Hypertension
- Hyperlipidemia
- Immunosuppression
- Depression
- Chronic obstructive pulmonary disease
- Gastroesophageal reflux disease
- Berger disease
- No known history of malignancy
Past Surgical History
- Living unrelated kidney transplant in 2012 for Berger disease (with immunosuppression)
Social History
Retired elevator mechanic with a history of asbestos exposure.
Medications and Allergies
Crestor, Imitrex, Nexium, Prograf, Labetalol
Allergy to Chlorhexidine, tape and Temazepam
Radiology
CT Findings: No definite adenopathy. Nodule in right lower lobe has increased in size from 1.4 x 0.9 cm to 2.0 x 1.2 cm.


Pathology
Cytology

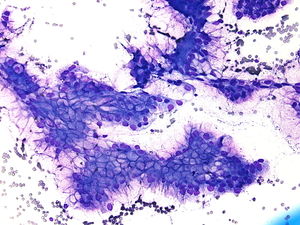
4x magnification of cohesive groups of cells that have hyperchromatic nuclei and have apical light colored vacuoles.
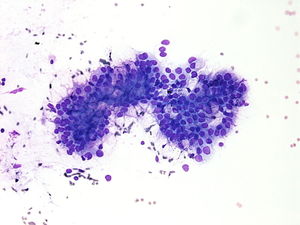
20x magnification of the same groups of cohesive cells. The apical vacuoles can be seen, and some of the nuclei are 4 times as large as the surrounding red blood cells in the background.
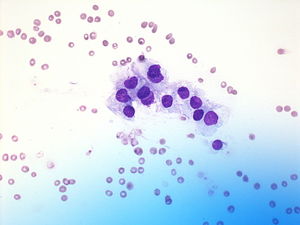
10x magnification of another cohesive group of cells. Again the apical vacuoles are present and the nuclei are large.
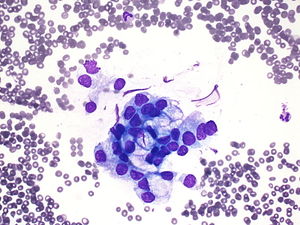
40x magnification of another group of cells. These cells have large hyperchromatic nuclei and have delicate cytoplasm.

4x magnification of a flat sheet of cells. The nuclei are larger than the surrounding red blood cells and scattered lymphocytes in the background.
40x magnification of a group of cells with hyperchromatic large nuclei and delicate cytoplasm.






Resident Questions
Biopsy Histology
- CytologicallyYoursCoW20131118Biopsy1.JPG
4x magnification of the lung biopsy specimen. The lower left side of the image displays more normal appearing histology while that in the upper right displays a more glandular histology.
- CytologicallyYoursCoW20131118Biopsy2.JPG
20x magnification of the glandular histology and mucin.
- CytologicallyYoursCoW20131118Biopsy3.JPG
40x magnification of glandular histology and mucin.
Final Diagnosis
Cytology
- Mucinous neoplasm present. This is a peculiar lesion consisting of mucinous atypical cells and pools of mucin. Consider low-grade mucinous neoplasm. Differential diagnosis includes bronchiolo-alveolar carcinoma vs. primary mucinous neoplasm of the lung vs metastasis from elsewhere.
Biopsy
- Mucinous adenocarcinoma (bronchioloaveolar carcinoma, mucinous type).
Case Discussion
This is a classic cytology and histology of a mucinous adenocarcinoma of the lung.