IPLab:Lab 11:Leishmaniasis
Contents
Clinical SummaryEdit
This 28-year-old white male presented to the dermatology clinic complaining of sores on his arms. On examination, two lesions measuring 0.7 to 1.5 cm in diameter were present on his right arm. These lesions showed central ulceration and a raised, indurated margin surrounding the ulcer. The lesions had developed over approximately one month. The patient had applied topical antibiotics, which had no effect. The patient had recently returned from a World Wildlife Fund study site in the Amazon region of Brazil, where he had been conducting field research in the rain forest. A biopsy was taken from the raised edge of one of the ulcers.
ImagesEdit

In this photograph of the skin lesion seen in this patient, note the raised edges (arrows) and the ulcerated center.
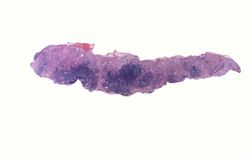
This is a low-power photomicrograph of the biopsy taken from this skin lesion. The ulcerated surface is at the top. Note that the specimen is heavily infiltrated with inflammatory cells.
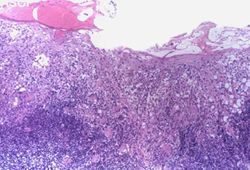
This is a higher-power photomicrograph of this biopsy. The ulcerated surface is seen on the top of the section. Again, note that the specimen is heavily infiltrated with inflammatory cells.
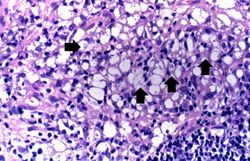
This high-power photomicrograph of the biopsy specimen shows more clearly the heavily infiltrate of inflammatory cells. Note the small blue structures inside the inflammatory cells (arrows).
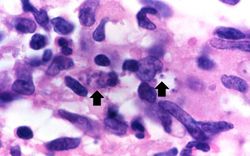
This is a high-power photomicrograph of an inflammatory cell containing cytoplasmic organisms (arrows).
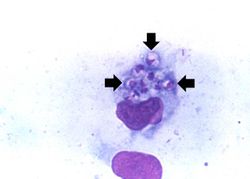
This is a high-power photomicrograph of a touch prep made from the skin lesion at the time of biopsy. A single macrophage can be seen with intracytoplasmic leishmania organisms (arrows).






Study QuestionsEdit
Additional ResourcesEdit
ReferenceEdit
- eMedicine Medical Library: Leishmaniasis
- eMedicine Medical Library: Leishmaniasis in Emergency Medicine
- eMedicine Medical Library: Dermatologic Manifestations of Leishmaniasis
- Merck Manual: Leishmaniasis
Journal ArticlesEdit
- Choi CM, Lerner EA. Leishmaniasis as an emerging infection. J Investig Dermatol Symp Proc 2001 Dec;6(3):175-82.
ImagesEdit
An infiltrate is an accumulation of cells in the lung parenchyma--this is a sign of pneumonia.